By Origen Kinesis
Do your patients experience shoulder or chest pain during bench pressing—even when their technique seems correct?
It’s more common than you think, especially in people who train regularly and perform repeated loaded pushing movements.
Interestingly, many of these cases aren’t due to traumatic injuries, but rather to a subtle issue often overlooked in clinical settings…
One of the most common mistakes is failing to assess the synergy between the pectoralis major and the serratus anterior.
When this relationship breaks down, movement becomes inefficient, compensations arise, and sensitive structures—such as the shoulder joint or the pectoralis tendon—get overloaded, eventually leading to pain.
Now, with surface electromyography (EMG), you can detect in real time whether both muscles are working as they should. That allows you to adjust exercises, select the right load, and retrain movement without worsening symptoms.
Want to learn how to integrate this tool into your clinical work?
👉 Get all the info about mDurance here and start making clinical decisions based on objective data.
In this post, you’ll find a step-by-step guide for assessing and retraining the pectoralis major–serratus anterior synergy during pressing movements.
What Should You Assess If You Suspect Pectoralis Major Tendinopathy?
Step 1: Evaluate the Pectoralis Major–Serratus Anterior Synergy
During the bench press (especially under moderate to heavy load), the ideal synergy is:
Pectoralis Major > Serratus Anterior
- Pectoralis major is the prime mover, generating the pushing force.
- Serratus anterior stabilizes the scapula throughout the movement, maintaining posture and movement efficiency.
When the serratus anterior doesn’t stabilize well, the pectoralis becomes less efficient and other muscles (like the anterior deltoid or elbow flexors) step in to compensate.
The result: overload, reduced performance, and increased injury risk.
Real Case: Patient With Pain and Diagnosed Pectoralis Major Tendinopathy
Upon analyzing the bench press movement with surface EMG, we observed:

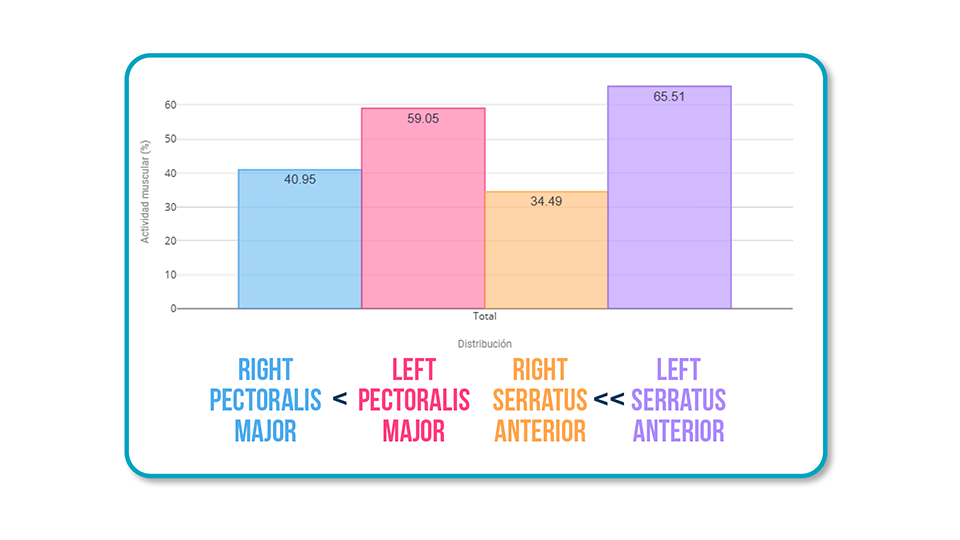
- Right pectoralis major < Left (X)
- Right serratus anterior << Left (X)
This led us to a clear conclusion:
The issue wasn’t just in the tendon—it was in the entire motor pattern.
Both the prime mover (pectoralis) and the key stabilizer (serratus) were underactive on the symptomatic side.
How to Retrain This Pattern Effectively
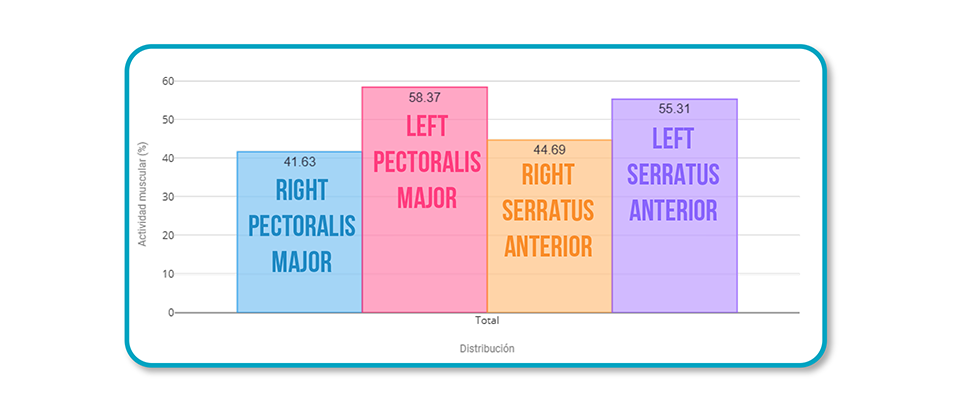
1. Dumbbell Bench Press

Advantage: Allows micro-adjustments in trajectory.
Result: Gradual increase in muscle activation, especially of the pectoralis major, without triggering pain.
✔️ Improves synergy without overloading painful structures.
✔️ Ideal during the early stages of rehab.
2. Kettlebell Bench Press

Advantage: Controlled instability → greater demand for active stabilization.
Result: More balanced activation between both sides.
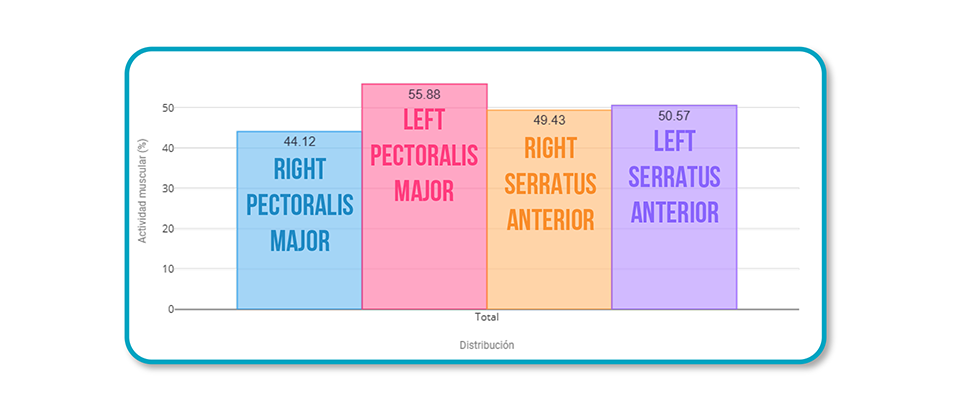
✔️ The patient must actively “control” the load, improving serratus anterior integration.
✔️ Useful for progressing toward more stable, functional patterns
So What Role Does EMG Play in All This?
Surface EMG enhances the way you assess and correct these types of injuries. With it, you can:
✅ Objectively measure activation of the pectoralis major and serratus anterior
✅ Detect muscular compensations before they become painful
✅ Retrain movement in real time with visual biofeedback
✅ Choose the exercises (and variations) that truly improve activation without worsening symptoms
Conclusion
Sometimes the solution isn’t removing an exercise—it’s adjusting how it’s performed.
A small variation in load (using dumbbells or kettlebells) and a better understanding of the muscular pattern can be the difference between chronic tendinopathy and efficient movement retraining.
And if you want to make clinical decisions based on data—not assumptions—EMG is the tool you need.
Want to see how EMG could help you treat patients with shoulder or chest pain?
👉 Get all the info about mDurance here and start designing treatments based on real data.

