Do you know which exercise generates the greatest pelvic floor activation?
It is probably not the one you have in mind.
If you work with athletes who experience urine leakage or incontinence symptoms, this article will help you design your training and rehabilitation programmes.
Because the problem is not just the incontinence. It is also not having an objective way to assess what is really happening in that musculature while your patient moves.
The problem that almost no one considers when prescribing pelvic floor exercises
Many women who practise high-impact sport present pelvic floor dysfunction. The data is more striking than may appear: up to 70% of young female athletes may have incontinence symptoms without having given birth.
And yet, in most cases, the training programme does not change. Not because the professional does not want to adjust it, but because they do not have objective data on which to base that decision.
Standard clinical tests do not always detect what is really happening. Subjective assessment has clear limitations. And without objective information about how the pelvic floor activates during each exercise, the consequences are direct:
❌ You design training programmes without a real understanding of the capacity of that musculature.
❌ Treatments rely on the patient’s subjective perception rather than measurable data.
❌ Your patient does not improve and you have no way of knowing exactly what to adjust.
This is where surface electromyography can make a real difference.
What EMG contributes to pelvic floor assessment
With electromyography you can evaluate the real activation of the intracavitary muscles of the pelvic floor in different exercises and movement conditions.
Not what should be happening according to theory, but what is actually happening in that specific patient, in that specific exercise.
This allows you to answer questions that would otherwise have no objective answer: is the pelvic floor really working in this position? Is the activation sufficient to generate adaptations? Is it ready to withstand the impact that the patient’s sport demands?
In a study that used the mDurance system to measure the activity of the intracavitary muscles of the pelvic floor in different positions and exercises, the results showed very clear differences between conditions. And some of those differences contradict the most common clinical intuition.
Which exercises activate the pelvic floor the most
The squat: the most effective exercise
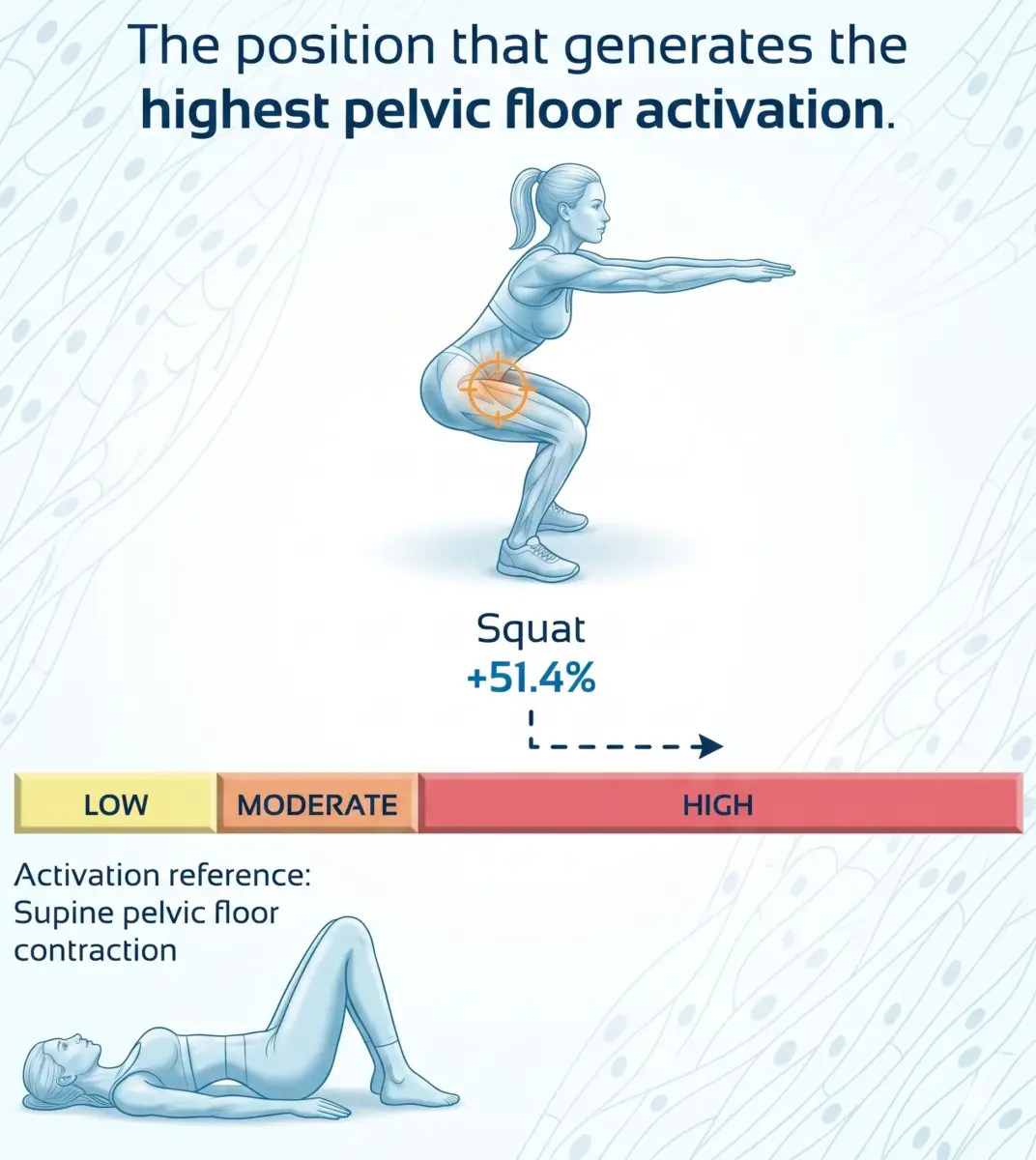
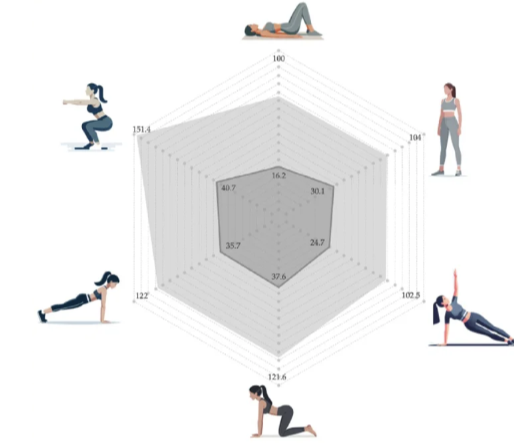
The squat is the position that generates the greatest pelvic floor activation, with a value of 151.4% relative to the reference contraction (this contraction is the maximum pelvic floor contraction in supine position).
In other words, in a squat the pelvic floor works considerably harder than at rest or in simple static positions.
This finding has a direct clinical implication: if your goal is to stimulate and strengthen the pelvic floor, the squat is one of the most efficient options available, provided the patient can perform it correctly and the musculature is in a condition to tolerate that demand.
Plank and four-point kneeling: also above the threshold
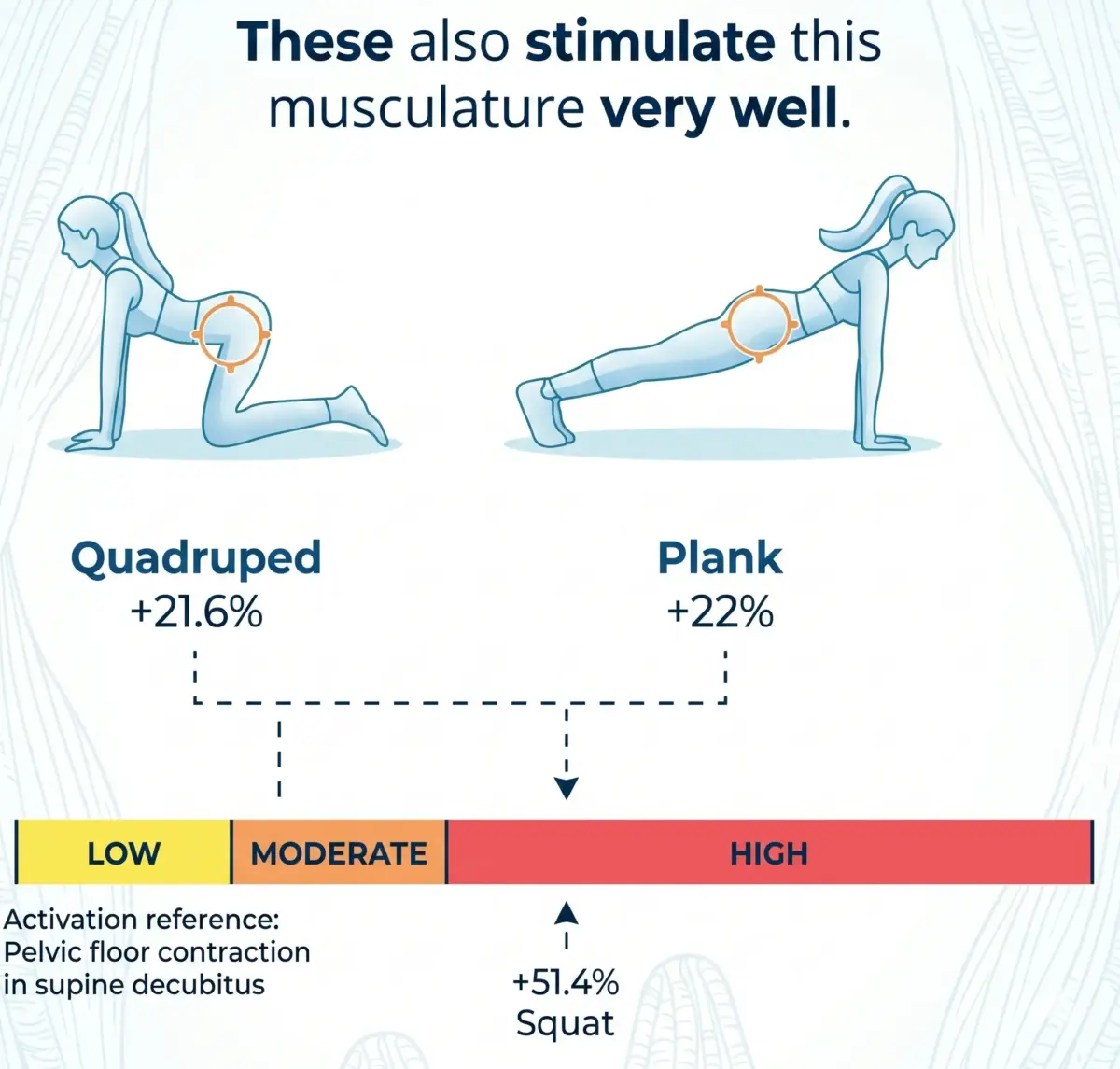
The front plank and the four-point kneeling position showed very similar activation level, both above the reference value:
- – Front plank: 122%
- – Four-point kneeling: 121.6%
Both positions challenge trunk and pelvic stability in a way that requires an active pelvic floor response. They are valid options for phases in which the squat is not yet tolerable or when a lower-intensity stimulus is sought.
The least effective options for pelvic floor strength training
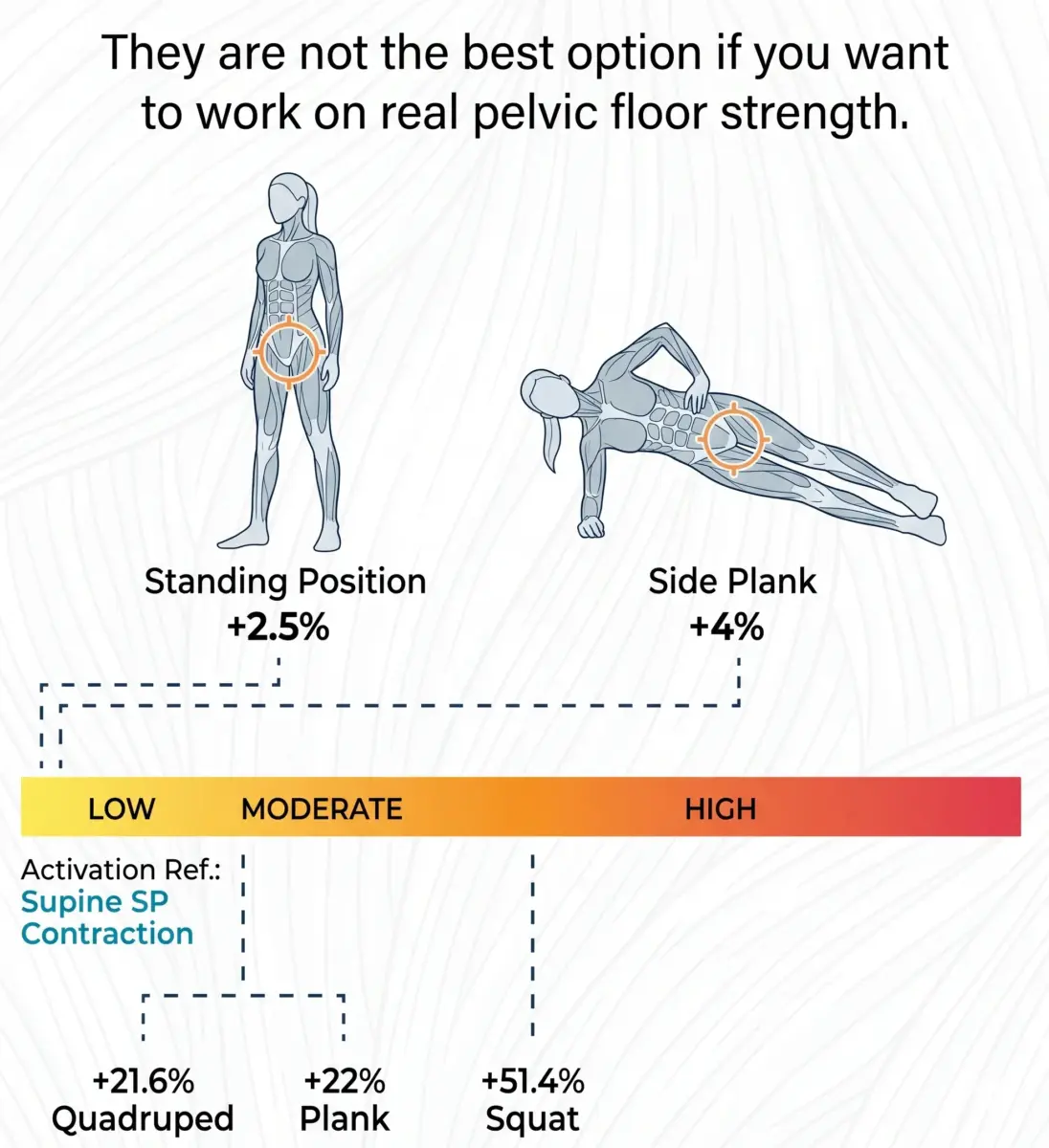
At the opposite end of the ranking, the lowest activation values corresponded to:
- – Supine position: 100% (baseline reference value)
- – Static standing: 104%
- – Side plank: 102.5%
These figures do not mean that these positions are incorrect or should be removed from the programme. They mean that, if the specific goal is to stimulate pelvic floor strength, these options generate a considerably lower stimulus than the squat or the front plank.
Why position matters so much
The pattern that emerges from this data has a clear biomechanical explanation: positions that challenge gravity and pelvic stability generate greater pelvic floor activation.
In a squat, the pelvis and trunk work through a range of motion that demands an active and coordinated response from the entire pelvic floor musculature to maintain continence and stability.
In supine position, that demand practically disappears because gravity no longer represents a challenge for that musculature.
This is precisely why many patients can activate the pelvic floor correctly in a lying position during clinical examination, but fail when they are standing, running or jumping.
How to use this information in your clinical practice
Knowing this data allows you to make far more precise decisions in three specific areas:
Personalise the plan according to the sport and the symptoms. A patient who practises yoga is not the same as one who runs 40 kilometres a week. The exercises in the programme should replicate the postural and activation demands she will encounter in her real sporting activity.
Assess with data whether the pelvic floor is ready to withstand impact. Before returning a patient to her sport, you can use EMG to verify that activation in loaded positions, such as the squat, reaches the levels needed to protect her during impact. Not as an estimate, but with real data.
Adjust loads and progressions safely. You can design a progression that moves through four-point kneeling and the plank before introducing higher-demand positions like squats. And you can verify in each session whether the progression is working.

