Do you have CrossFit patients with shoulder pain that do not improve even though they have strength and there is no structural injury?
The problem is probably not in the tissue. It is in how the neuromuscular system controlling that shoulder is organised.
This article analyses a study that measured the effect of a single session of electrical peripheral neuromodulation on mobility, strength and scapular motor control in CrossFit athletes.
The results challenge the standard approach to non-specific shoulder pain and open a very specific clinical pathway for treating it with data.
Why shoulder pain in CrossFit is not just a mechanical problem
In non-specific shoulder pain in CrossFit, load is not the only factor. What usually fails is neuromuscular control, scapular coordination and the ability to regulate muscle tension after fatigue.
This is why some shoulders do not tolerate more load even when they have strength: the problem is not contractile capacity, but how the system is organised to produce movement.This has a direct implication for treatment: if the problem is one of neuromuscular organisation, adding more load without correcting that organisation not only fails to help but can perpetuate the dysfunctional pattern.
What the study found in “healthy” athletes
The study started with a sample of 40 CrossFit athletes with no known structural injury. Despite being considered healthy, the majority presented measurable alterations:
- ❌ Loss of internal rotation mobility in 35.7% of cases.
- ❌ Strength deficit in both internal and external rotation.
- ❌ Clear inhibition of the lower trapezius and serratus anterior.
- ❌ Hyperactivity of the upper trapezius.
In other words: a shoulder that moves, but is poorly organised. With strength, but with an activation pattern that under fatigue or overhead load becomes a real risk factor.
The question guiding the study was not “how do I remove the pain?” but something more precise: can neuromodulation change measurable risk factors?
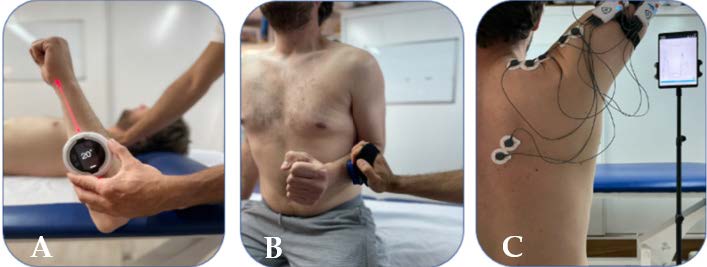
To answer it, mobility, strength and scapular motor control were assessed with EMG, before and immediately after the intervention.
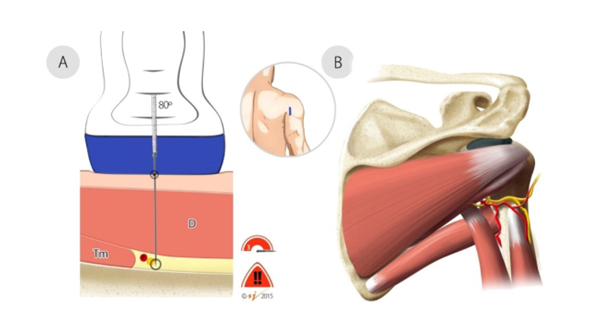
The intervention: a single session of electrical peripheral neuromodulation (EPN)
The intervention consisted of a single session of electrical peripheral neuromodulation (EPN) targeting the axillary and suprascapular nerves, with the following parameters:
- – Biphasic stimulation.
- – 10 stimuli of 10 seconds with 10-second rest intervals between them.
- – Pulse width of 240 μs.
- – Intensity sufficient to generate a pain-free contraction.
- – Frequency of 10 Hz, which produced the best results.
One single session. No additional exercise. Neuromodulation only, to isolate its effect on each variable.
Results by variable
Variable 1: Mobility
Mobility was the parameter most sensitive to the intervention. After a single EPN session:
- ✅ Internal rotation of the treated shoulder increased.
- ✅ Total range of motion increased.
- ✅ Improvement was seen even in the untreated shoulder, suggesting a central modulation effect, not only a peripheral one.
Mobility is the first parameter to respond to neural modulation. This makes sense: internal rotation restrictions in overhead athletes frequently have a neuromuscular rather than structural component.
When the nervous system reduces the “brake” on movement, range improves before any change occurs in the tissue.
Variable 2: Strength
Changes in strength were more limited. Only external rotation improved, and the ratio between external and internal rotation did not normalise after the session.
The conclusion is direct: neuromodulation does not replace training. It is not a tool for generating strength. It is a tool for improving the conditions in which training will act.
Variable 3: Scapular motor control
This is the most clinically relevant result. EPN managed to reduce upper trapezius activation in the athletes assessed.
In CrossFit athletes who regularly perform overhead movements, the upper trapezius tends to be hyperactive. That hyperactivity competes with the infraspinatus, serratus anterior and lower trapezius, worsens scapular mechanics and intensifies under fatigue. Reducing it is not an aesthetic goal: it is the necessary condition for the stabilising muscles to do their job properly.
Neuromodulation, in this context, acts as a re-education window. It lowers the noise of the upper trapezius and creates space for the right exercise to activate what needs to be activated.
The real clinical value: the neuromuscular reset
Neuromodulation is not the final treatment for these patients. Its clinical value lies elsewhere: it acts as a partial neuromuscular reset that reduces upper trapezius interference and creates more favourable conditions for subsequent motor re-education.

Put another way: first you modulate, then you train. And when you train in that state, the exercise is more likely to activate the muscles you need to activate because the compensatory pattern is temporarily reduced.This is precisely the moment where EMG shifts from being a diagnostic tool to being a treatment tool. You can verify in real time whether, after neuromodulation, the lower trapezius and serratus anterior respond better to exercise. And you can adjust the exercise based on what you see, not on what you assume.
How to combine EMG and neuromodulation in your clinical practice
The combination of both tools allows a very concrete workflow:
Before neuromodulation: you measure with EMG the activation of the upper trapezius, lower trapezius, serratus anterior and infraspinatus during reference exercises. You have the baseline.
After neuromodulation: you repeat the same assessment. If the intervention has worked, the upper trapezius activity decreases and the stabilisers have more response capacity. You have the objective data confirming that the re-education window is open.
During subsequent exercise: you use real-time EMG to choose which exercise activates the lower trapezius or infraspinatus most with the least upper trapezius interference. You do not guess which exercise works best for that patient: you verify it.
The result: greater activation of the muscles that protect the shoulder, lower activation of the hyperactive upper trapezius and an objective way to demonstrate progress session by session.
Frequently asked questions
Is EPN the same as percutaneous electrolysis or dry needling? No. Ultrasound-guided peripheral neuromodulation acts on the peripheral nerve, not on muscle tissue or tendon. Its mechanism of action is different: it modulates neural excitability and the organisation of the muscle activation pattern, rather than generating a local inflammatory response.
Is a neuromodulation session needed before every exercise session? Not necessarily. The goal is to open a re-education window that allows exercise to reorganise the motor pattern. Over time, that pattern consolidates and dependence on neuromodulation decreases. Frequency depends on the individual patient’s response.
Does it work the same way in patients with structural injury? The study was conducted with athletes with no known structural injury. In patients with rotator cuff tears, glenohumeral instability or other structural injuries, the clinical approach is different. Neuromodulation may play a complementary role, but it does not replace the specific management of the injury.
Can I apply this protocol without EMG? You can apply EPN without EMG, but you lose the ability to verify whether the intervention is having the desired effect on scapular motor control. Without EMG, you do not know whether the upper trapezius has reduced its activation or whether the lower trapezius is responding better to exercise. You are working blind on the variable that matters most in these patients.
Conclusion
Non-specific shoulder pain in CrossFit athletes frequently has a neuromuscular component that neither strength nor imaging can explain. A poorly organised shoulder, with an overactive upper trapezius and inhibition of the lower trapezius and serratus, does not improve with more load alone.
Ultrasound-guided peripheral neuromodulation offers a pathway to reorganise that pattern before training. A single session can improve mobility, reduce upper trapezius activation and open a re-education window where the right exercise has greater impact.
EMG gives you the data to verify that window is open, to choose the exercise that best takes advantage of that moment and to demonstrate progress objectively.
Treat. Measure. Train. With data from the very first session.

