When you think about rehabilitation after an ACL injury or surgery, which muscles come to mind?
Quadriceps, hamstrings, gastrocnemius. The standard protocol. But there is a muscle that directly conditions knee biomechanics during every landing and that is rarely measured objectively: the gluteus medius.
And when it does not activate properly, the knee pays the price.
In this article you will discover what is really happening in the gluteus medius and the adductors during a single-leg landing in patients with reconstructed ACL, why that pattern is not detected with the naked eye and which five parameters you should be measuring before clearing a patient to return to sport.
Why the gluteus medius is key in ACL rehabilitation
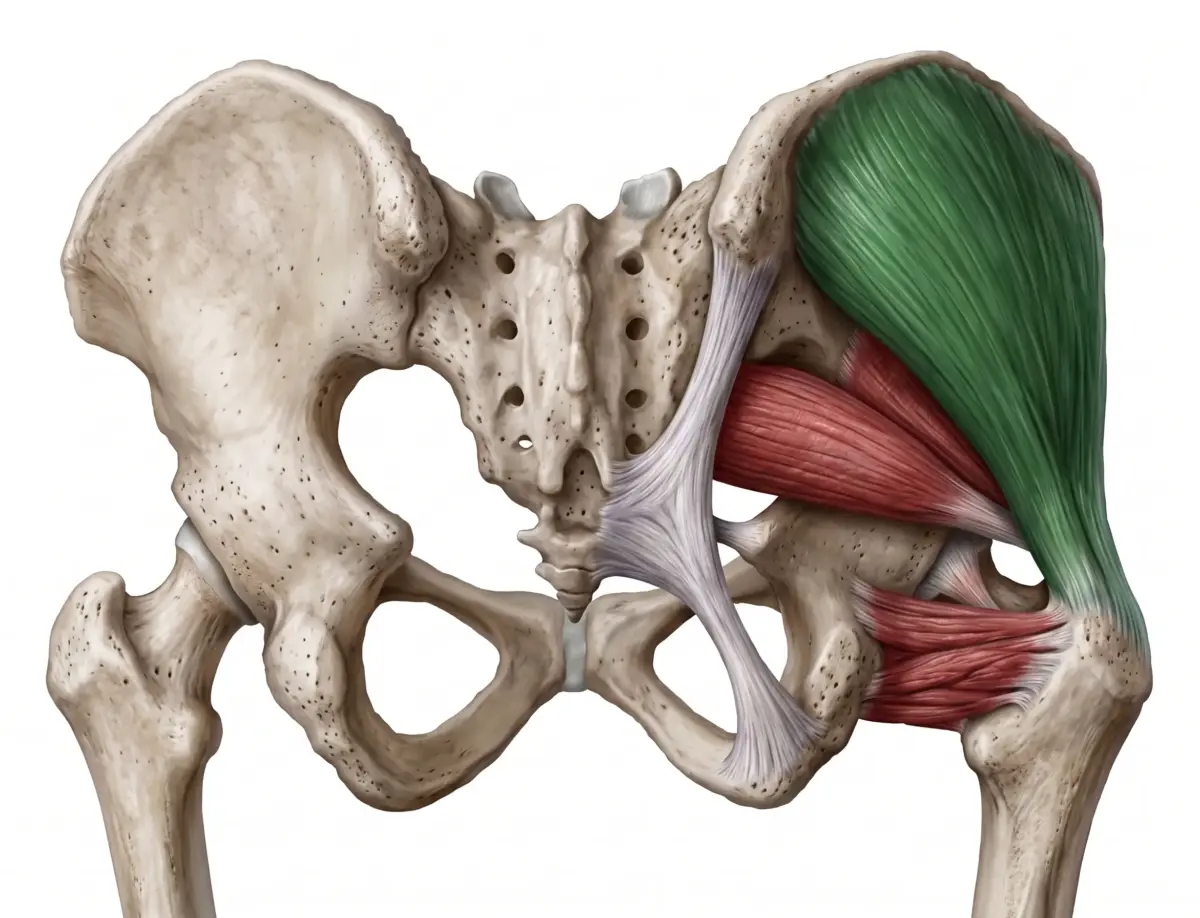
The gluteus medius controls three fundamental things during a jump landing:
- – Pelvic stability in the frontal plane.
- – Femoral rotation and adduction.
- – Resistance to dynamic knee valgus.
When it fails, the pattern most associated with ACL injuries and re-injuries appears: hip adduction combined with knee valgus at the moment of impact.
This is not a theory. It is the most documented biomechanical mechanism in the literature on ACL injuries.
The problem is that this pattern is difficult to observe clearly with the naked eye during a landing. It happens in milliseconds. And the difference between a gluteus medius that responds and one that does not can be invisible in standard clinical observation.
The study: what was measured and in whom
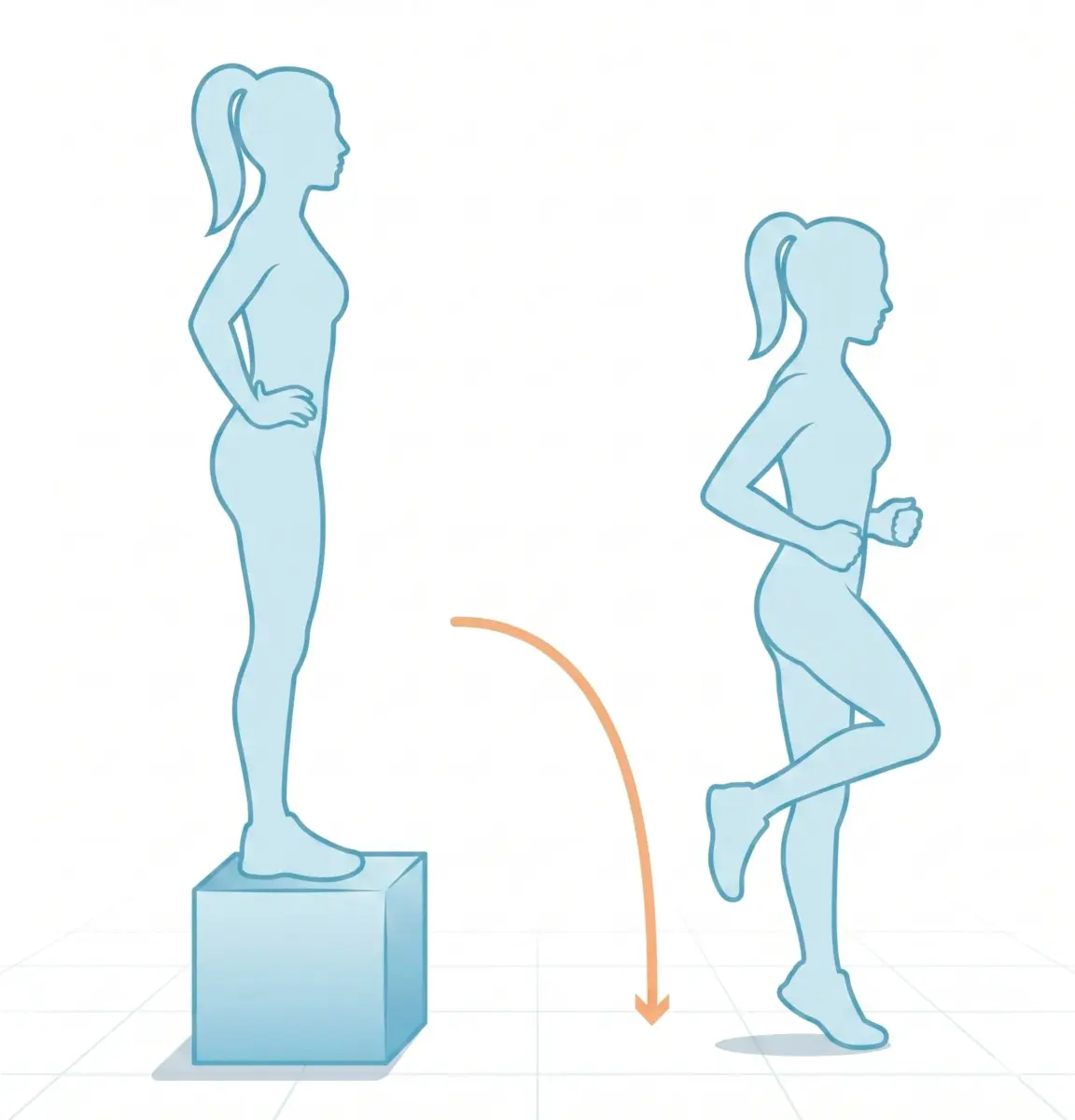
In a study that evaluated muscle activation during a single-leg drop landing, patients with reconstructed ACL were compared against healthy subjects.
The variables measured with EMG were:
- – Gluteus medius activation (GMED).
- – Adductor longus activation (AL).
- – GMED:AL coactivation ratio (interpreted as the division between gluteus medius activation and adductor longus activation).
- – Reactive response of both muscles in the first milliseconds after ground contact.
Two findings stood out above the rest.
Finding 1: the gluteus medius responds poorly after contact
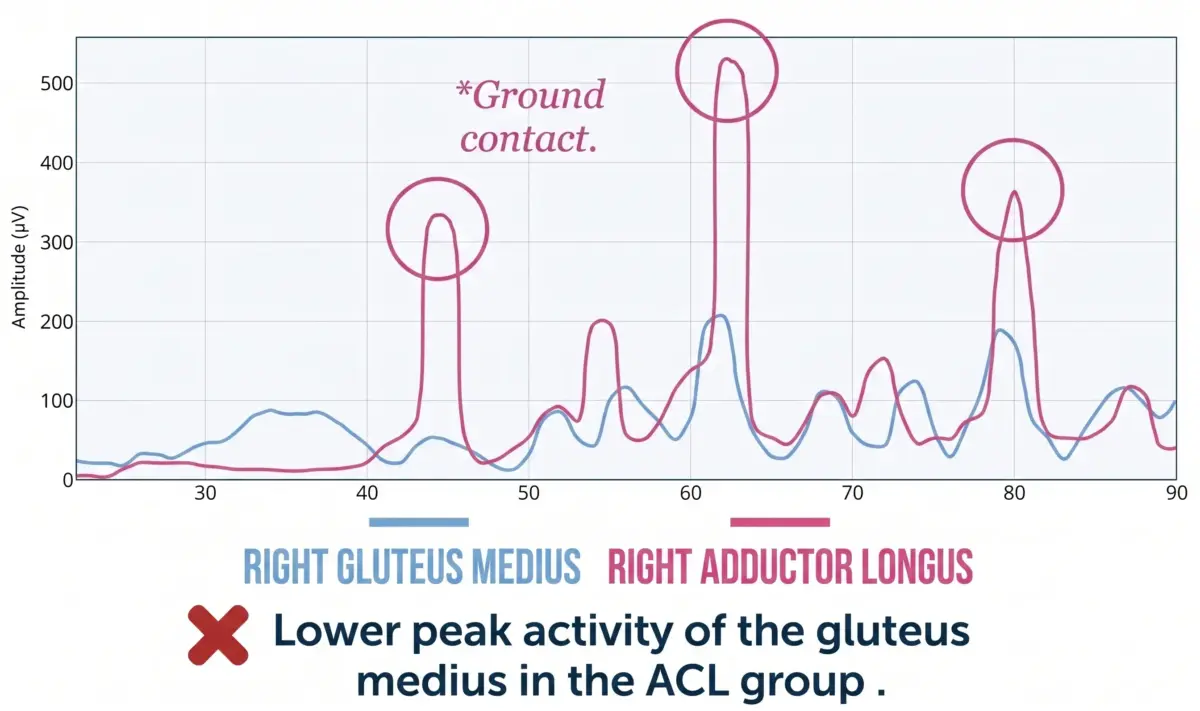
In the reconstructed ACL group, the peak activity of the gluteus medius after ground contact was significantly lower than in the healthy group.
We are not talking about the maximum strength of the muscle under controlled conditions, but about its reactive response capacity at the critical moment of landing.
The clinical implications are direct: less gluteus medius activation at that instant means less capacity to restrain femoral adduction and internal rotation, which translates into greater knee valgus and greater load on the ACL with every landing.
A patient may have good gluteus medius strength in isometric tests or in controlled exercises and still have this reactive deficit in dynamic situations.
Without measuring the movement with EMG, you will not detect it.
Finding 2: the gluteus medius – adductor synergy is altered
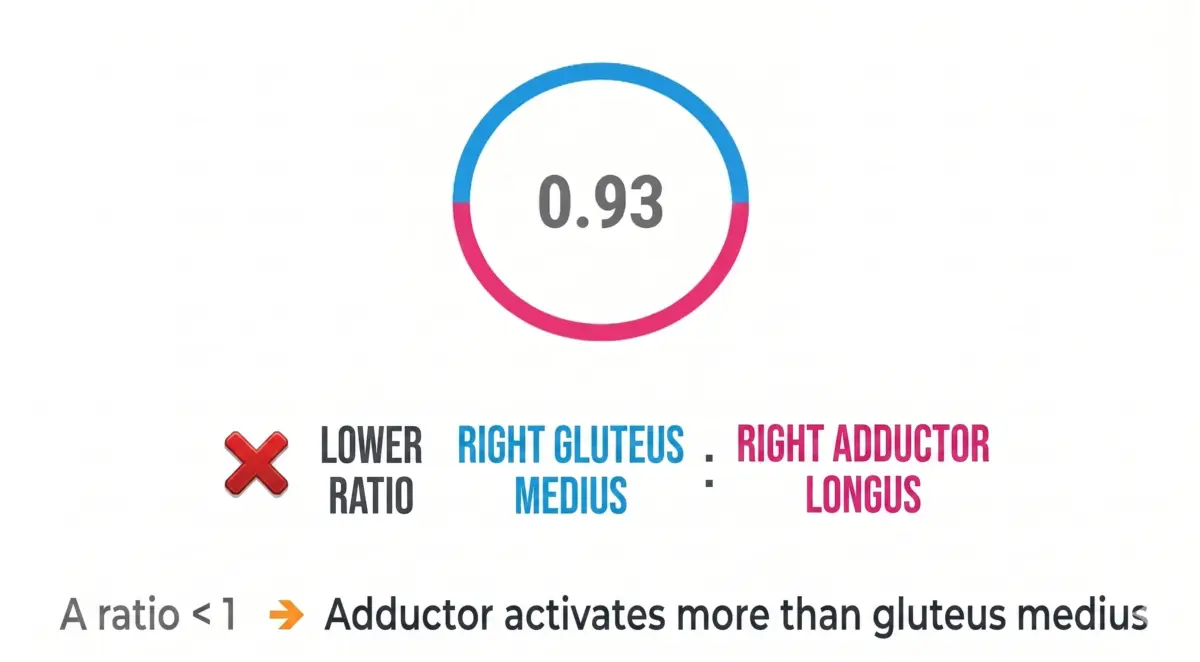
The second finding is even more relevant from a motor control perspective: patients with reconstructed ACL showed a lower GMED:AL ratio than healthy subjects.
A ratio below 1 means that the adductor longus activates more than the gluteus medius during the landing. The muscle that drives the pelvis towards valgus is leading the task over the muscle that should be restraining it.
In practice, this translates into a medial collapse pattern: the adductors organise the movement and the gluteus medius does not generate a sufficient response to counteract it. The result is exactly the biomechanical pattern of greatest risk for the ACL.
Why this pattern occurs
The causes of this deficit are not solely related to strength. They are related to neuromuscular organisation:
- – Gluteus medius weakening through disuse or reflex inhibition following the injury or surgery.
- – Decreased central drive, meaning reduced recruitment from the central nervous system as an adaptive response to pain or injury.
- – Motor control changes that become established after the injury and are not automatically corrected when strength is recovered.
- – Poorly organised reactive movement. The muscular response to impact is an automatic process that requires specific training. If not explicitly addressed, the compensatory pattern learned during the injury persists.
- – Consolidated compensatory strategies. The nervous system learns to move differently to protect the injured knee. Those strategies do not always disappear once the structure has recovered.
This pattern is not visible to the naked eye. EMG shows it to you in seconds.
What you should be evaluating in your ACL patients
If you work with patients in rehabilitation following ACL injury or surgery, these are the parameters you should be measuring during jumps and landings:
1. Reactive activation of the gluteus medius. Not its maximum isometric strength, but its response in the first milliseconds after contact. This is the variable most directly related to re-injury risk.
2. GMED:adductor longus ratio. A ratio below 1 indicates that the adduction/medial collapse pattern is active. It is the signal that the rehabilitation programme needs to intervene specifically on this synergy.
3. Femoral control in the frontal plane. Combining EMG data with movement observation allows you to determine whether the neuromuscular deficit is translating into a visible biomechanical alteration.
4. Pelvic stability in the first 200-300 ms. The anticipatory and reactive response of the pelvis at the moment of landing is the most sensitive indicator of hip neuromuscular control.
5. Lumbopelvic compensations. When the gluteus medius does not respond, other muscles compensate. EMG allows you to identify which muscles are taking on that load and whether the compensatory pattern is generating new risks.
Frequently asked questions
When is the right time to assess these parameters in an ACL patient? From the moment the patient can safely perform a single-leg landing, which generally coincides with the mid or late stages of rehabilitation. Early assessment of these patterns allows you to detect deficits before the patient returns to high-impact sporting activity.
Can a patient with good gluteus medius strength still have this deficit? Yes, and this is one of the most common errors in ACL rehabilitation. Strength under controlled conditions does not guarantee an adequate reactive response in dynamic situations. These are different capacities that require specific assessment and training.
How is the reactive response of the gluteus medius specifically trained? Through exercises that simulate real reactive demand: single-leg landings, direction changes, plyometric exercises with visual or tactile feedback. Real-time EMG allows you to verify whether the muscle is responding at the right moment and with the appropriate magnitude, and to adjust the exercise based on that data.
Does this pattern normalise on its own over time after surgery? Not necessarily. Studies on post-ACL rehabilitation show that motor control deficits can persist even after clinical discharge and return to sport if not specifically addressed. Recovery of muscle strength and recovery of motor control are parallel processes that require differentiated intervention.
Conclusion
ACL rehabilitation does not end when the quadriceps recovers its strength. It ends when the neuromuscular system returns to organising movement safely in high-demand situations, such as landing from a jump.
The gluteus medius and its relationship with the adductor longus are two of the most relevant variables in that process and two of the least measured in standard clinical practice. Not because they are unimportant, but because without EMG they are almost invisible.
Measuring the reactive activation of the gluteus medius, the GMED:adductor ratio and pelvic stability in the first 200-300 ms after contact gives you a picture of motor control that no strength test can provide.
And that picture is exactly what you need to know whether your patient is ready to return to their sport, or whether the pattern that put them at risk the first time is still there.

