And stop treating low back pain blindly
Many patients with low back pain come to your clinic convinced that “the problem is in the back.”
They point to the area, describe stiffness, talk about tightness… and expect you to work directly on the lumbar region.
But in a large percentage of cases, the origin is not only in the spine.
👉 It’s in the hip.
When the gluteus maximus and gluteus medius fail to generate sufficient force or lack proper coordination, the lumbar area takes on a role it shouldn’t: excessive stabilization and extension.
The result is a very common pattern:
Reduced glute activation → Increased lumbar activation → Overload → Recurrent pain.
If you don’t detect this altered synergy, you can spend weeks treating the consequence instead of the cause.
In this post, you’ll find a 15-minute protocol to assess glute–lumbar synergy in a structured and actionable way starting today.
By the way, how many of your patients with low back pain are you treating without analyzing their glute-lumbar pattern?
What does the literature say about low back pain and gluteal musculature?
Evidence shows a clear association between low back pain and alterations in:
- – Gluteus maximus.
- – Gluteus medius.
- – Spinal erectors.
But there’s an important nuance:
We’re not always talking about pure weakness. Often, the issue is neuromuscular discoordination.
That means:
- ❌ Muscles that activate too late.
- ❌ Muscles that activate too much.
- ❌ Muscles that activate in the wrong phase.
Your job is not just to “strengthen.” It’s to detect which muscle is overworking and which one is underperforming.
Practical 4-test protocol (15 minutes)
You can apply this protocol during the first assessment session.
Test 1: Glute bridge
Objective: Identify gluteal weakness and excessive lumbar co-activation.
What to observe:
- – Does the patient feel more load in the lower back than in the glutes?
- – Is there excessive lumbar extension?
- – Is there paravertebral trembling or rigidity?
Typical altered pattern:
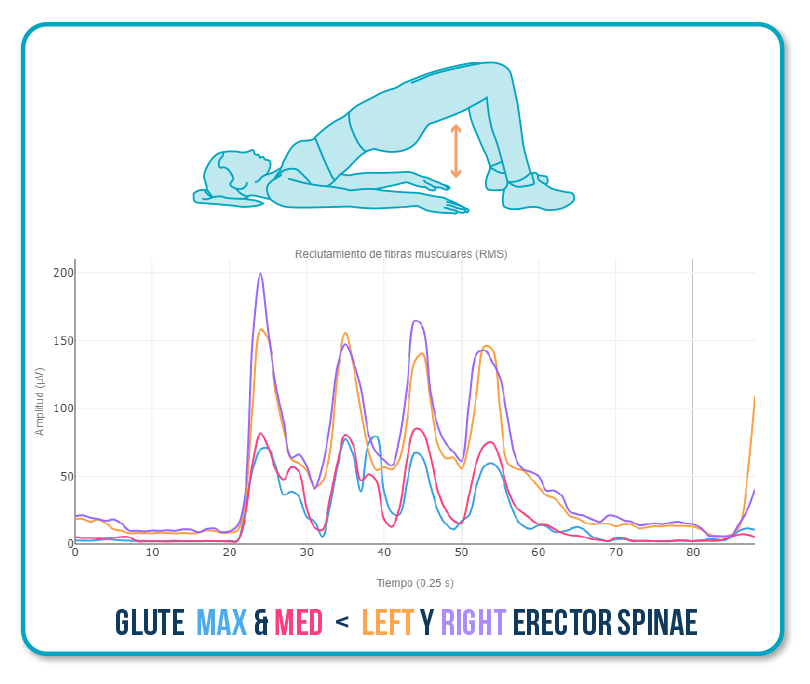
This indicates that extension is being generated from the spine instead of the hip.
TIP for re-education:
- – Reduce range of motion.
- – Add tactile feedback on the glutes.
- – Use EMG biofeedback so the patient learns to increase glute activation without increasing lumbar activity.
Test 2: Hip abduction
Objective: Detect gluteus medius deficit and lumbar compensation.
Red flags:
- – Trunk lean.
- – Compensatory external rotation.
- – Premature lumbar activation.
Typical altered pattern:
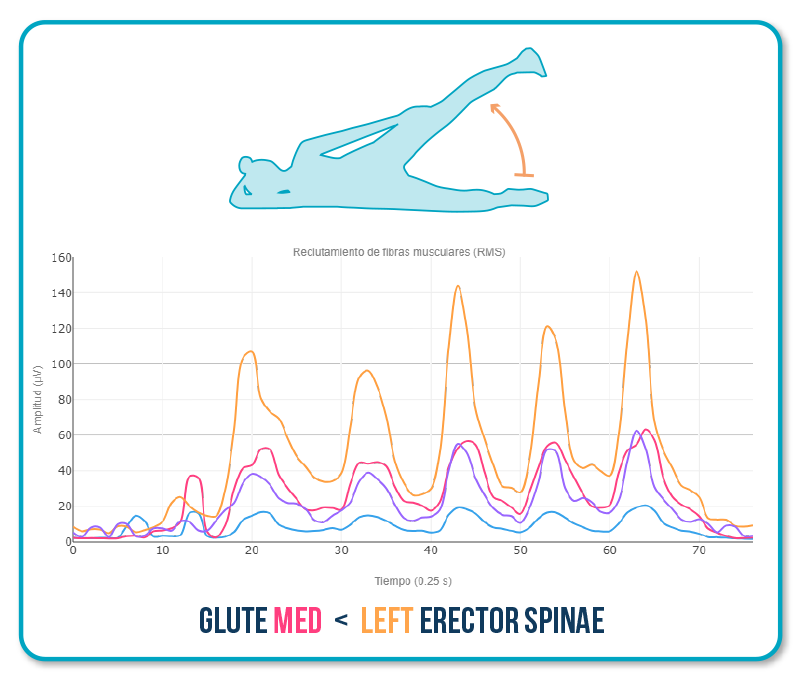
When the gluteus medius does not stabilize the pelvis, the trunk leans to the opposite side and the lumbar region compensates.
Test 3: Single-leg squat
Objective: Analyze dynamic coordination between glutes and erectors.
This functional test reveals the real load-bearing pattern.
Observe:
- – Pelvic drop.
- – Excessive lumbar flexion.
- – Paravertebral dominance.
Typical altered pattern:
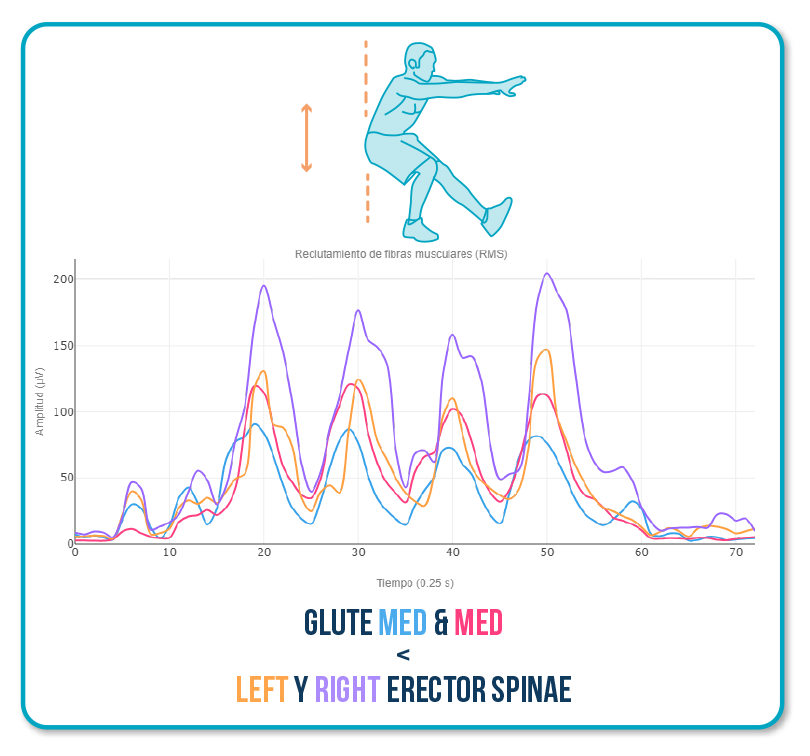
Here, the patient stabilizes from the spine instead of the hip.
Test 4: Cat-Camel
Objective: Identify lumbar deficit and lumbopelvic discoordination.
Altered pattern:
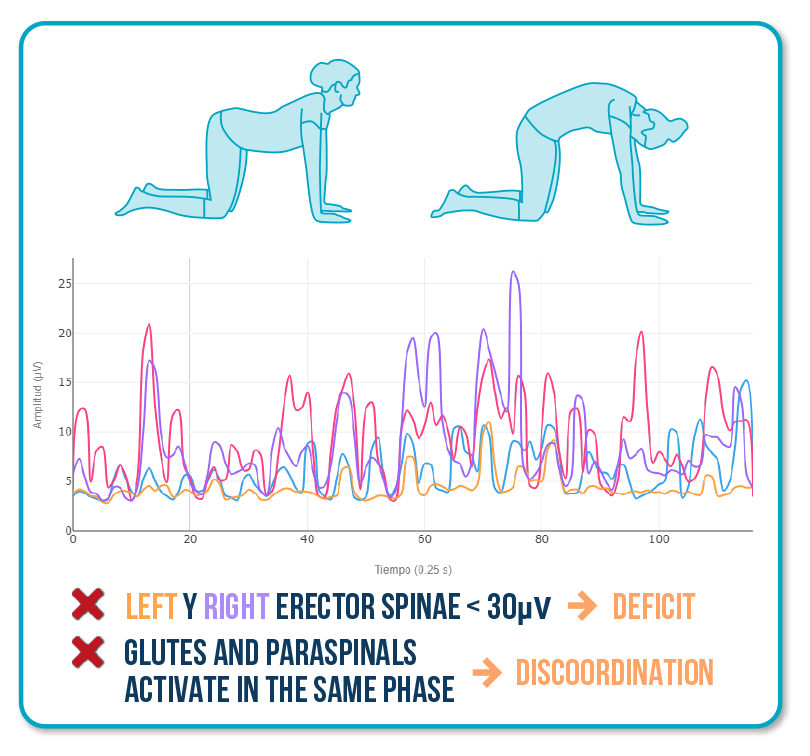
Here, the issue is not strength, but segmental control.
Intervention:
- – Segmental lumbar activation.
- – Lumbopelvic rhythm training.
- – Slow, conscious progression.
What changes when you measure with EMG?
With electromyography, you can clearly see:
- ✅ Which muscle is compensating.
- ✅ When it activates.
- ✅ In which movement phase.
- ✅ How it changes after re-education.
That transforms your intervention:From assumption → to validation.
From intuition → to objective data.
From “I think it’s improving” → to “glute activation has improved by 20%.”
Why this protocol saves you weeks of treatment
If you don’t assess glute-lumbar synergy, you risk reinforcing compensations without realizing it. You might be strengthening the back when you should be re-educating the hip. You might even be progressively increasing load before coordination between the glutes and lumbar region has improved.
The problem isn’t that the patient isn’t working.
The problem is that they may be working with the wrong pattern.
When you detect the altered pattern from the beginning, everything changes. You adjust earlier, correct earlier, and progress earlier. That translates into less recurrent pain, fewer relapses, and better clinical outcomes in less time.
Stopping blind treatment doesn’t mean applying more techniques. It means understanding which muscle is failing in the synergy and correcting it with precision.

