Review these muscles and movements
After an ankle injury, many patients recover their range of motion and apparent strength within a few weeks. They may walk without pain, perform basic exercises, and even return to some sports activities.
However, despite this apparent recovery, a significant number of them continue to report a feeling of instability, insecurity when bearing weight, or frequent recurrences.
This happens because ankle recovery does not depend only on muscle strength. It also depends on how the muscles that stabilize the joint coordinate during functional tasks.
If this neuromuscular coordination is not properly restored, the ankle may appear to function well in isolated tests but fail when the foot is under load.
One clear example is the relationship between the peroneus brevis and the lateral gastrocnemius.
In this post you will learn how to assess the synergy between the peroneus brevis and the lateral gastrocnemius in patients with ankle injuries.
The synergy between the peroneus brevis and the lateral gastrocnemius
The synergy between the peroneus brevis and the lateral gastrocnemius is essential for ankle stability. In a healthy ankle, these two muscles work together to stabilize the joint during walking, running, or any single-leg support task.
The peroneus brevis plays a key role in lateral ankle control. It contributes to foot eversion and acts as a dynamic stabilizer that prevents inversion collapse, which is especially important after a lateral ankle sprain.
The lateral gastrocnemius participates in propulsion during the push-off phase and also contributes to ankle stability when the foot is in contact with the ground.
When both muscles work in coordination, the ankle can absorb load, stabilize during single-leg support, and generate propulsion efficiently. The problem appears when this synergy is altered.
What Happens When the Peroneus Brevis Fails
After a sprain or repeated episodes of instability, the peroneus brevis may lose activation capacity during functional tasks. Although the muscle can still contract during isolated tests, its response during functional movements may become reduced or delayed.
When this happens, the body attempts to compensate for the lack of stability by activating nearby muscles more strongly. In this situation, the lateral gastrocnemius often assumes part of the stabilizing role that should be performed by the peroneus brevis.
This compensatory strategy has several consequences. The ankle loses part of its lateral control, the load distribution pattern becomes less efficient, and the joint becomes more vulnerable to unexpected movements. Over time, this situation may lead to chronic instability, frequent recurrences, or a persistent feeling of insecurity when bearing weight.
To identify these alterations, evaluating muscle strength on the treatment table is not enough. It is necessary to analyze how the muscles behave in different movement contexts.
Clinical Case: Patient With Pain in the Right Ankle
A typical clinical case involves a patient who comes to consultation after an ankle injury. During the initial examination, the pain is moderate and the range of motion appears almost normal. However, the patient reports instability during more demanding tasks such as jumping.
To understand what is really happening, muscle activation can be analyzed through three tests that explore different levels of neuromuscular demand.
First Test: Isometric Eversion
The first test consists of an isometric ankle eversion, used to determine whether the peroneus brevis can activate properly when the movement is isolated.
In this situation, activation of the right peroneus brevis was almost identical to the left side. No relevant differences were observed between the ankles.
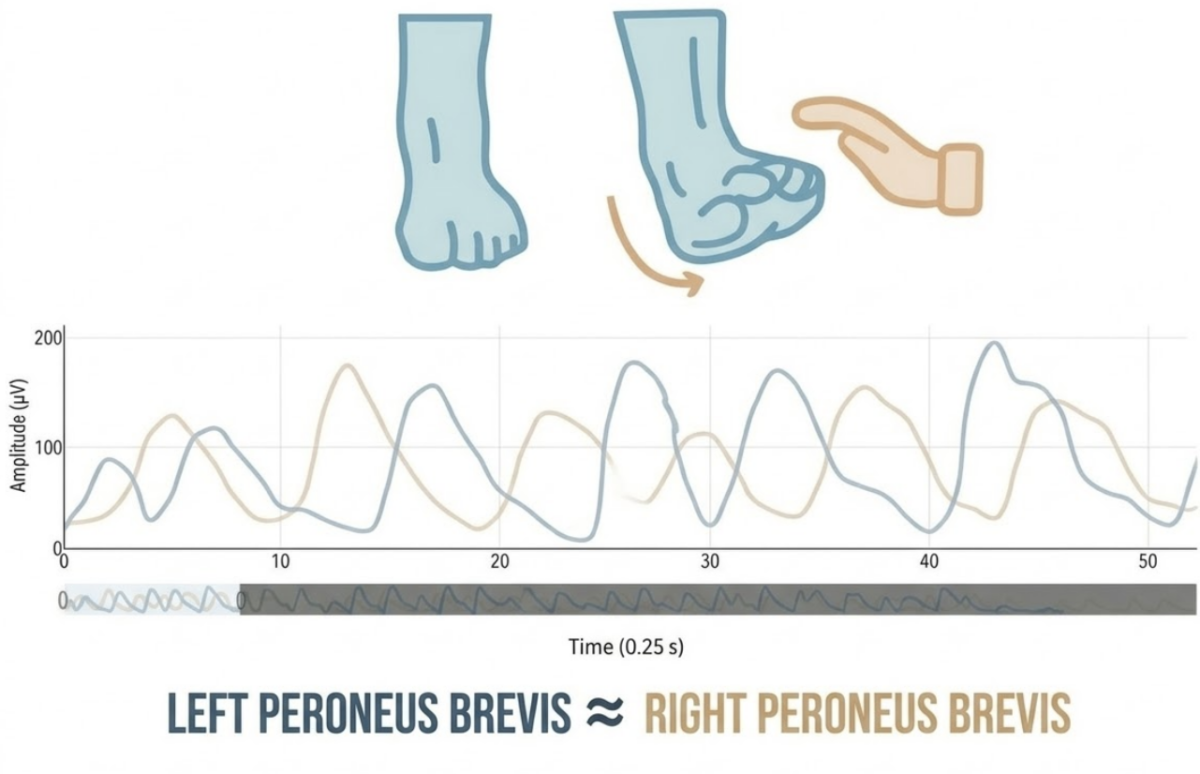
At first glance, this result might suggest that the muscle is functioning normally. However, this test is performed without load and in a very controlled environment, which does not always reflect the functional reality of the ankle.
Second Test: single-leg stance
The second test involves maintaining a single-leg stance, a situation that more closely resembles the real demands of walking or sport.
In this position, the ankle must stabilize body weight while the neuromuscular system continuously adjusts muscle activity to maintain balance.
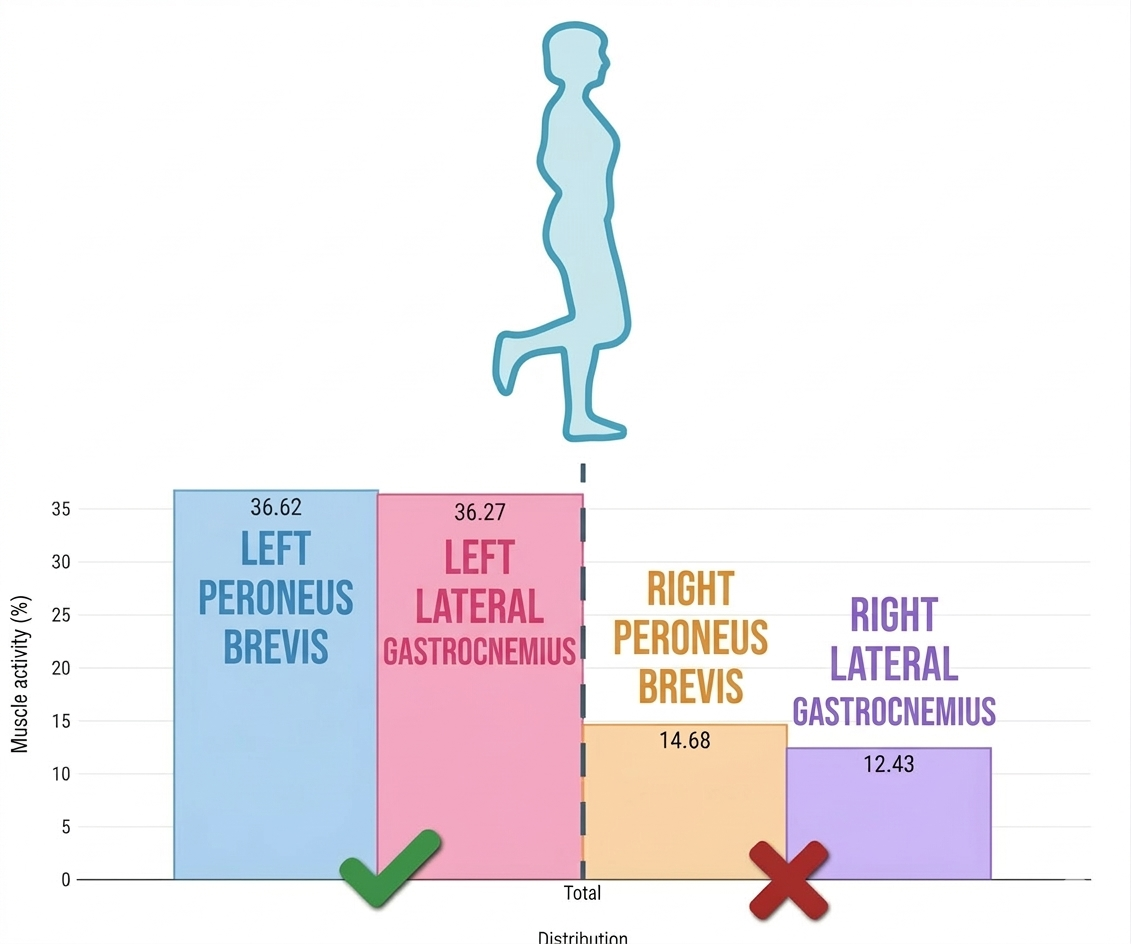
Here the first relevant finding appears: the right peroneus brevis shows an activation deficit, accompanied by reduced participation of the lateral gastrocnemius. This indicates that the neuromuscular system is not generating the appropriate response to stabilize the ankle under load.
Even though the muscle can activate during an isolated test, when the foot contacts the ground the neuromuscular response becomes insufficient.
Third Test: single-leg heel raise
The third test consists of a single-leg heel raise, a movement that demands greater participation from the gastrocnemius and also challenges ankle stability during propulsion.
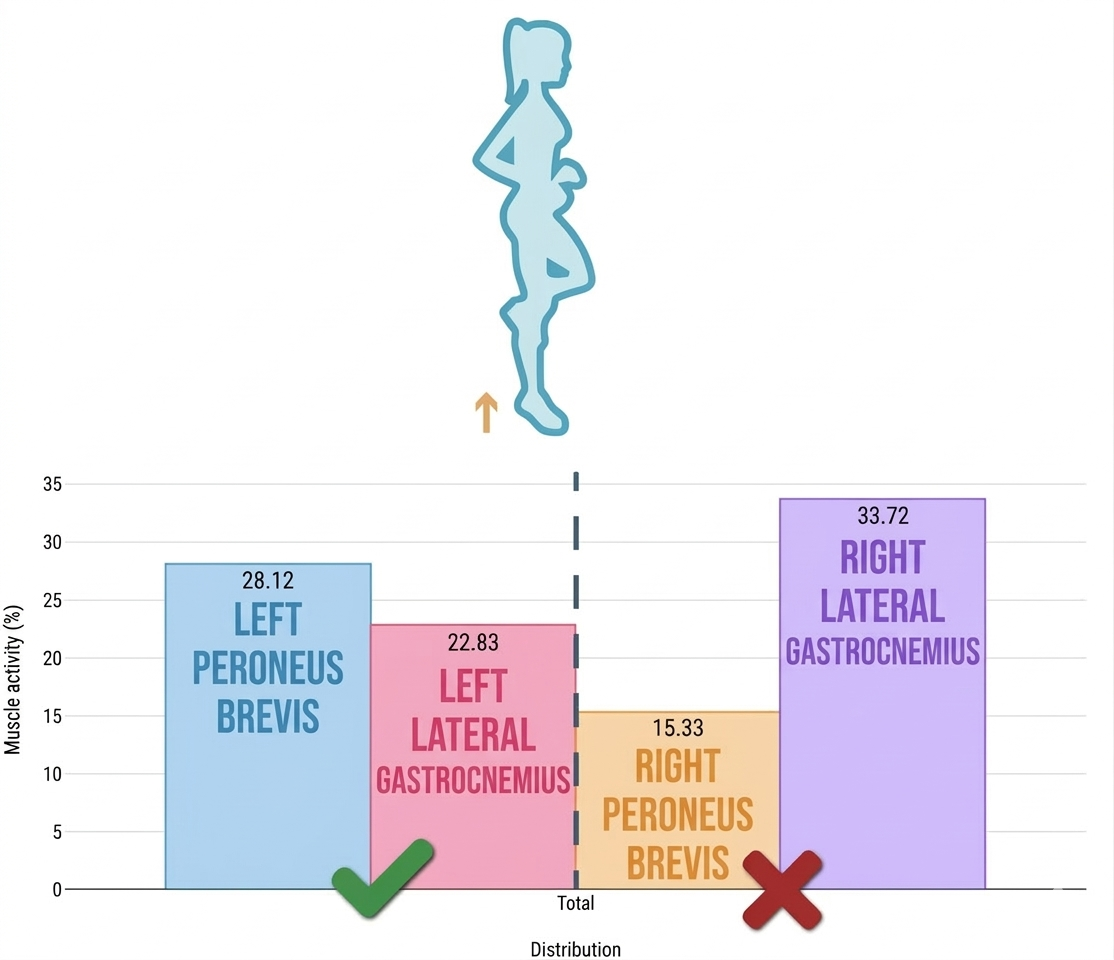
In this task a different pattern appears. The lateral gastrocnemius attempts to compensate for the deficit in the peroneus brevis by increasing its contribution to the movement. However, the right peroneus brevis continues to show lower activation than expected.
This suggests that the ankle is using a compensatory strategy to generate force, but it is not resolving the main problem: the lack of lateral stability.
Clinical Interpretation
These results illustrate something that occurs very frequently in clinical practice. A muscle may activate correctly in an isolated test and still fail when the movement becomes functional.
When the foot is on the ground, the neuromuscular system must integrate proprioceptive input, postural control, and coordination between different muscle groups. If one of these elements fails, ankle stability is compromised.
This is why a patient may show good results during table-based testing but still feel unstable when walking or running. Assessment must go beyond isolated tests and analyze muscle function in contexts that resemble the real demands of movement.
Why It Is Important to Detect These Deficits
If these deficits are not detected early, the patient may progressively return to activity with an inefficient activation pattern. This increases the risk of new injuries and promotes the development of chronic instability.
Treatment may also focus only on restoring general strength without addressing the neuromuscular coordination that is actually failing. The consequence is that the ankle appears to recover, but the problem returns as soon as load or speed demands increase.
Surface electromyography allows you to observe when and how strongly the muscles involved in ankle stability activate during different movements.
With this information you can detect deficits that do not appear in conventional tests and verify whether the rehabilitation exercises you prescribe are producing the neuromuscular response you expect.
Instead of relying only on the patient’s perception or external observation, you can objectively analyze muscle activation and adjust the treatment accordingly.
Conclusion
After an ankle injury, recovering mobility and strength does not always mean that neuromuscular function has been fully restored. In many cases the problem lies in how muscles coordinate when the foot contacts the ground.
Analyzing the synergy between the peroneus brevis and the lateral gastrocnemius allows you to identify compensatory patterns that may go unnoticed in a conventional assessment.
When these alterations are detected early, it becomes possible to design treatment strategies aimed at restoring real ankle stability and reducing the risk of recurrence.
Electromyography facilitates this process by objectively showing which muscles are working correctly and which ones need to be retrained to restore stable and efficient function.
Here is an important question: how many ankle recurrences occur because no one ever analyzed how the stabilizing muscles actually activate?
If you do not know which muscle is compensating and which one is failing, it becomes much easier for the patient to get injured again.

