Are your patients with shoulder pain not improving as expected?
You already know that subacromial syndrome is one of the most common shoulder conditions and a frequent source of pain. And while clinical diagnosis may seem straightforward, the true cause of the pain often remains hidden.
Many times, pain persists despite treatment, and you might ask yourself: Am I missing something important?
The answer could lie in imbalances within the scapulohumeral synergy, especially between the anterior deltoid, upper trapezius, and lower trapezius. Without analyzing these, you risk applying exercises that don’t fix the problem or even make it worse.
This is where surface electromyography (sEMG) comes in: a tool that shows you clearly how muscles behave during real movement. No more guessing, you can now measure, compare, and intervene with precision.
Imagine being able to see if your patient is overusing the anterior deltoid during arm elevation, or if the lower trapezius is barely active. Now you can, with objective data that sharpens your clinical reasoning.
👉 Want to learn how to detect these patterns and use data to guide treatment?
Book a free 10-minute call with an EMG expert physiotherapist. Zero pressure, fully personalized.
With this hands-on guide based on sEMG, you’ll be able to identify key muscular imbalances and design truly effective treatments for your shoulder pain patients.
Step 1: Identify the Symptoms That Give You Clues
Before placing electrodes or doing any instrumental assessment, listen to your patient.
What they often say:
- – “It hurts to lift my arm overhead.”
- – “My shoulder feels weaker.”
- – “I struggle to dress or reach up.”
What should you suspect?
These are classic signs of subacromial syndrome, but they also suggest a disruption in the synergy between movers (like the deltoid) and scapular stabilizers (like the upper and lower trapezius).
Step 2: Assess Shoulder Flexion with EMG and Observe the Motor Pattern
One of the most useful tests is having the patient actively flex the shoulder up to 180º (or to the pain-free limit) while recording muscle activity with surface EMG.
Place the electrodes on:
- – Anterior deltoid (primary mover)
- – Upper trapezius (scapular elevator)
- – Lower trapezius (scapular stabilizer and rotator)
Goal: Analyze how these muscles interact during the painful movement.
Step 3: Know the Typical Dysfunctional Patterns
What can go wrong?
- Overactive anterior deltoid:
If it activates too early or strongly, it pushes the humeral head upward and narrows the subacromial space, leading to pain on elevation. - Dominant upper trapezius:
Causes premature or excessive scapular elevation, leading to poor scapular rotation and added tension in the neck and subacromial space. - Inhibited lower trapezius:
Without its stabilizing and rotating action, the scapula remains in a suboptimal position for overhead movement, worsening the impingement.
These are compensatory patterns, not mistakes by the patient—and if you don’t identify them, corrective exercises may fail.
Step 4: Analyze the Results Using Real Clinical Examples
Example 1: Overactivation of Anterior Deltoid and Upper Trapezius
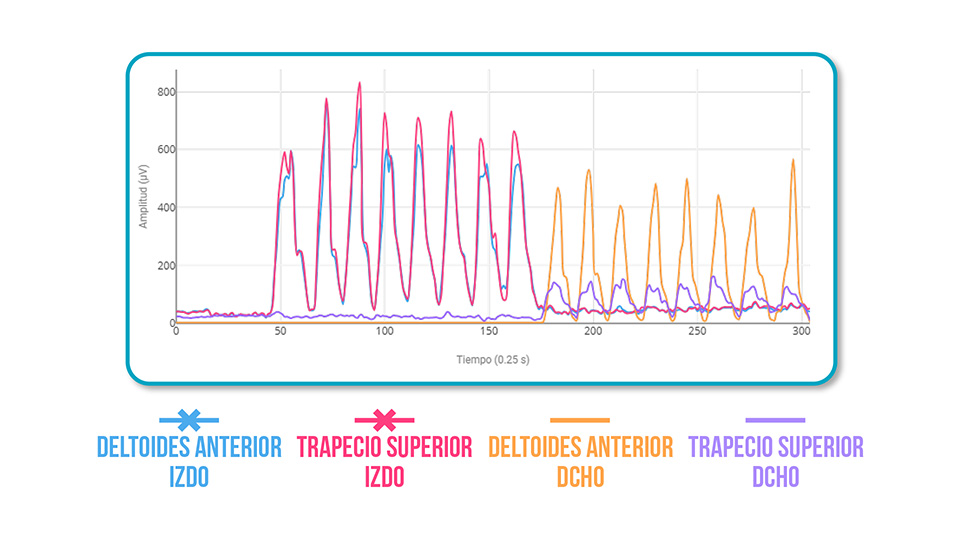
❌ Left upper trapezius hyperactivity → Increased neck and scapular tension
❌ Left anterior deltoid hyperactivity → Elevated subacromial pressure during arm raise
Example 2: Lower Trapezius Inhibition
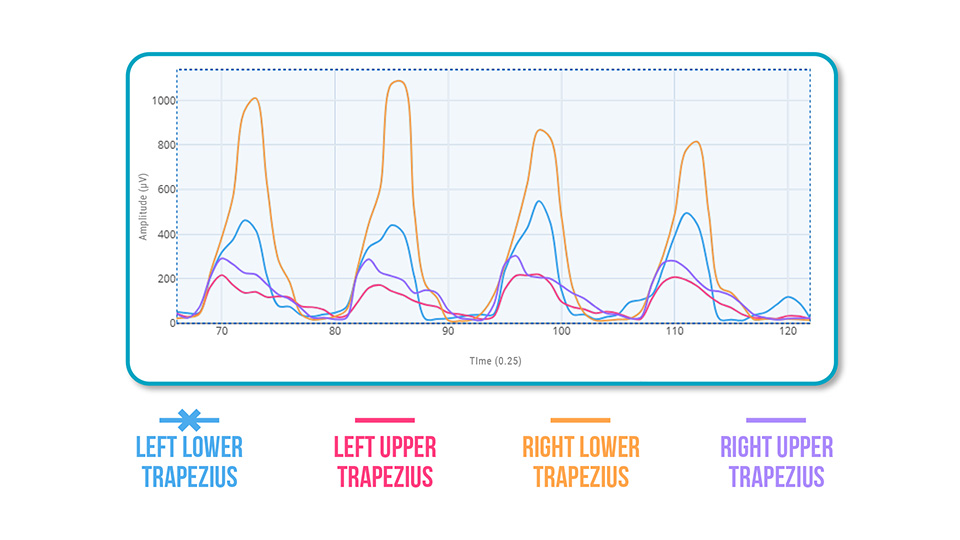
❌ Left lower trapezius deficit → Insufficient scapular rotation
Step 5: What Should You Look For with EMG?
✅ Ideal neuromuscular patterns:
- Lower trapezius: Progressive and sustained activation that stabilizes and rotates the scapula
- Upper trapezius: Moderate activation without excessive spikes
- Anterior deltoid: Firm but well-coordinated activation with scapular stabilizers
❌ Compensations to correct:
- Upper trapezius dominance
- Lower trapezius inhibition
- Deltoid overactivation without scapular control
Conclusion
Surface EMG doesn’t just confirm your clinical suspicions—it reveals what you can’t see: how muscles share the workload and who’s overcompensating.
When you evaluate subacromial syndrome with a functional and objective lens, you can:
- – Correct dysfunction at its source
- – Personalize exercises and avoid overload
- – Speed up recovery and reduce pain
Want to integrate surface EMG into your clinical practice?
Contact us here and discover how mDurance helps you make decisions based on real muscle data.
See you in the next post 🙂

