Do you work with athletes who play tennis or other asymmetric sports?
If so, there is a pattern you are probably seeing in your practice without always having an objective way to quantify it: the middle and lower trapezius loses its role in scapular stabilisation, and other muscles compensate for what it should be doing.
In this article you will learn what the science says about how muscle activation is altered in tennis players, which muscles fail first and which exercises have proven effective for retraining scapular function.
The problem with asymmetric sports
In sports such as tennis, the body adapts to years of unilateral dominance. Those adaptations are not always positive. What typically happens is:
⚠️ Marked dominance of one side over the other.
⚠️ Unequal muscle activation between the dominant and non-dominant limb.
⚠️ Progressive overload of the stabilising muscles, especially the trapezius and serratus anterior.
Over time, these adaptations increase the risk of shoulder injuries. They are also associated with a decrease in motor control and a drop in performance: less consistent strokes and early fatigue.
The muscle that loses the most function in this process is the middle and lower trapezius. And when that muscle fails, others take over its role compensatorily, which perpetuates the imbalance.
What the study with mDurance revealed
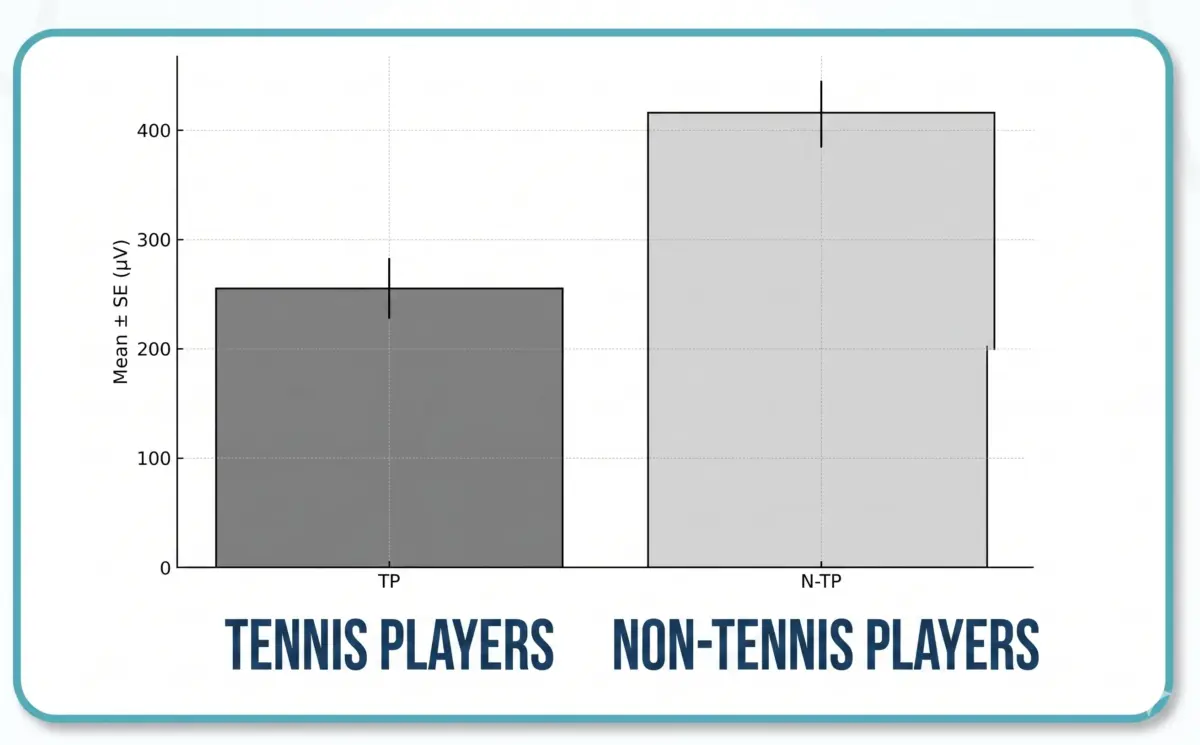
In a study that compared tennis players with athletes from symmetric sports using the mDurance system, the activation of the middle and lower trapezius was measured during scapular stabilisation exercises.
The results were consistent:
Lower activation of the middle and lower trapezius in tennis players compared to the symmetric sports group. This difference was not visible to the naked eye during exercise execution, but EMG quantified it with precision.
Compensatory use of the deltoid and spinal erectors. When the middle and lower trapezius do not generate sufficient activation, other muscles take on that load. The result is an inefficient movement pattern that perpetuates the asymmetry and increases the risk of injury.
Interscapular muscle asymmetry in both exercises assessed. The difference between the dominant and non-dominant side was consistent, confirming that the asymmetric adaptation affects scapular function bilaterally, not only on the striking side.
The most effective exercises for retraining the middle and lower trapezius
Exercise 1: Prone scapular retraction with feet elevated

Clinical goals:
- ✅ Activate the middle and lower trapezius in a loaded position.
- ✅ Stabilise the scapula at maximum retraction.
- ✅ Engage the core through foot elevation, increasing the overall stabilisation demand.
The prone position eliminates deltoid compensation and forces the trapezius to be the primary muscle of scapular retraction.
Foot elevation adds an additional stabilisation demand that better replicates the real effort conditions of the athlete.
Exercise 2: Bilateral scapular retraction with resistance bands in standing
Clinical goals:
- ✅ Control the retraction throughout the full range of motion, not only at the end point.
- ✅ Improve scapular and respiratory coordination during movement.
- ✅ Retrain interscapular symmetry by working both sides simultaneously.
Band work in standing allows progressive resistance adjustment and better replicates the postural demands of sport. Bilateral execution makes it easier for the athlete to perceive and actively correct the difference between both sides.
What you gain when you assess and train with EMG
Incorporating EMG into the assessment and training of asymmetric athletes gives you three specific advantages:
Knowing exactly which side fails and at which angle of movement. Not all trapezius deficits present in the same way. EMG shows you whether the problem lies in the initial phase of the movement, at the point of maximum retraction or in the eccentric control of the return.
Selectively activating the muscles that protect the shoulder. With real-time data you can adjust the position, load or execution until the middle and lower trapezius generates the activation you need, without relying on the patient’s subjective perception.
Reducing injury risk and improving stroke efficiency. When the trapezius correctly stabilises the scapula, the rotator cuff works under optimal mechanical conditions. This translates into less overload, better force transfer and greater consistency in performance.
Frequently asked questions
Does this pattern of scapular asymmetry appear only in tennis players? No. It is especially common in asymmetric sports such as badminton, padel or handball. Any sport that involves repetitive one-sided dominance generates similar adaptations in middle and lower trapezius activation.
How do I know if my patient has a middle or lower trapezius deficit without EMG? Clinical tests such as resting scapular position assessment, dyskinesis evaluation or the Kibler test can guide the diagnosis, but they do not quantify real activation during movement. EMG adds the dynamic dimension that static tests cannot provide.
When should these exercises be introduced into the programme? It depends on the recovery or prevention phase the athlete is in. Prone retraction is a good starting point because it minimises deltoid compensation. Progressing to band work in standing makes sense once control in prone is consistent.
Is it also necessary to work the serratus anterior? Yes. The serratus anterior and the lower trapezius work together to control scapular rotation. A lower trapezius deficit without addressing the serratus can generate a different compensatory pattern. EMG allows both muscles to be assessed simultaneously and the programme to be designed based on which one is most limiting scapular function.
Conclusion
In asymmetric sports, the middle and lower trapezius is the muscle that most frequently loses efficiency. That loss is not visible to the naked eye, but it can be measured with EMG and corrected with the right exercises.
Prone scapular retraction and bilateral band retraction are two data-backed options for retraining that function. But their real effectiveness in each patient can only be verified by measuring.
Assessing with EMG means knowing which side fails and at which angle. Training with that data means less risk and better performance.

