Functional assessment in people with cerebral palsy has traditionally been based on clinical scales and subjective observation. These tools are useful, but they have an important limitation: they do not always reflect what is actually happening at the muscular level.
This creates a double problem. On one hand, there may be errors in the classification of muscular status in cerebral palsy. On the other hand, training may be designed based on assumptions that do not match the patient’s neuromuscular reality.
The key question is clear: what if you could objectively measure which muscles are working, how they work, and when they fail?
The value of measuring muscle activity instead of assuming
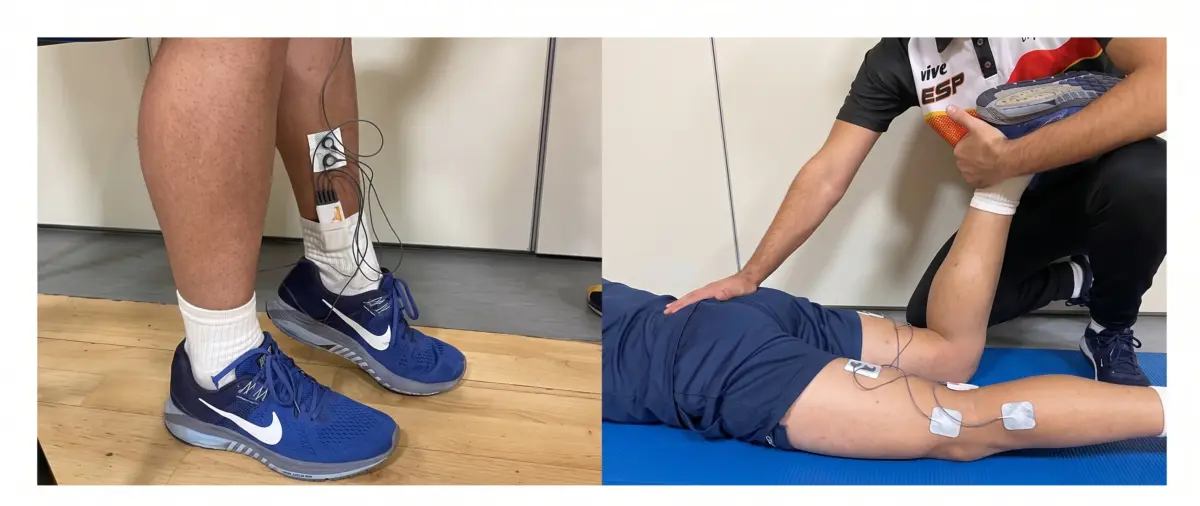
Surface electromyography (EMG) allows you to analyze the electrical activity of the muscle both at rest and during contraction. This provides information that cannot be obtained through observation alone.
Thanks to EMG, you can determine whether a muscle is hyperactive at rest, whether it can activate when required, or whether there are significant differences between both sides of the body.
This type of information is especially relevant in people with cerebral palsy, where muscle patterns are often altered by phenomena such as spasticity, excessive coactivation, or poor neuromuscular efficiency.
What really happens in the muscle: a practical case
In an EMG analysis, patients with cerebral palsy were compared to healthy individuals. Three key muscles involved in performance and lower limb stability were evaluated: the soleus, adductor magnus, and biceps femoris.
The assessment was carried out in two very specific situations: at rest and during a maximum isometric contraction.
This approach makes it possible to understand not only how much a muscle can activate, but also how it behaves when it should be relaxed.
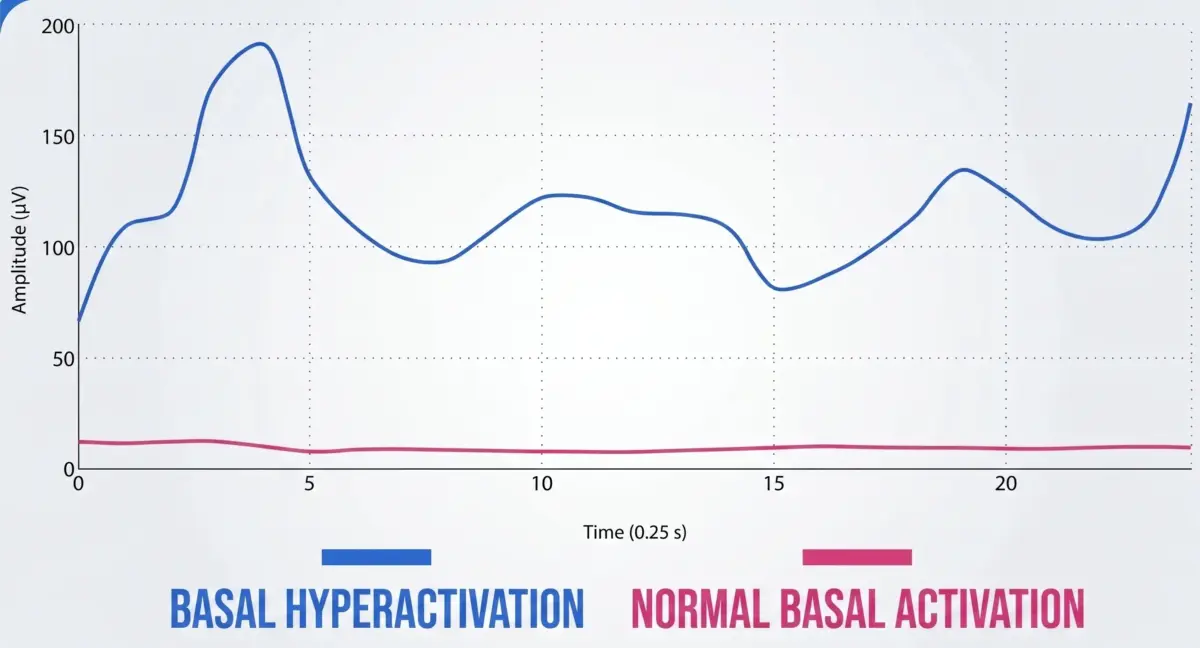
Key finding at rest: muscle hyperactivity
One of the most relevant findings was that, in patients with cerebral palsy, the muscles on the affected side showed elevated activity even at rest.
This means that the muscle is not truly relaxed when it should be. There is an increase in baseline muscle tone, reflecting the presence of spasticity or constant neuromuscular activation.
From a clinical perspective, this has important implications. A muscle that is continuously active:
- ❌ Fatigues earlier,
- ❌ Consumes more energy,
- ❌ Loses the ability to respond efficiently.
In addition, this baseline hyperactivity can interfere with the ability to generate an effective voluntary contraction when movement is required.
Second finding: reduced activation during maximal contraction
When patients were asked to perform a maximal contraction, something seemingly contradictory occurred. Muscles in individuals with cerebral palsy showed lower activation compared to healthy patients.
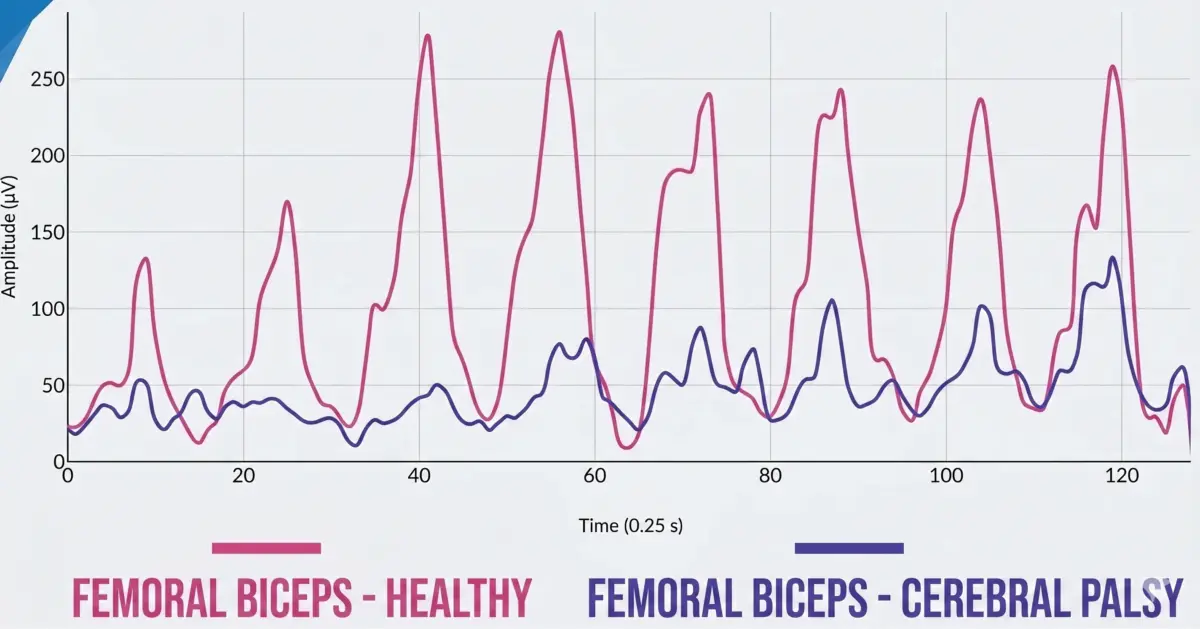
This indicates that, although the muscle is more active at rest, it is not capable of generating sufficient activation when it is actually needed.
This phenomenon reflects low neuromuscular efficiency. The muscle is constantly “on,” but does not respond adequately when demanded.
The key combination: spasticity + low efficiency
The combination of both findings defines one of the most characteristic patterns in cerebral palsy:
- ❌ Higher baseline activity.
- ❌ Reduced voluntary activation capacity.
This results in a muscle that works more than necessary but produces less than it should.
From a functional perspective, this has clear consequences.
When a muscle presents this pattern, the patient loses the ability to generate force efficiently. Power decreases, movement becomes less coordinated, and symmetry between both sides is disrupted.
This not only affects performance, but also increases the risk of injury. A neuromuscular system that does not respond efficiently is more vulnerable to loads, changes of direction, or unexpected situations.
In addition, these types of alterations are not always visible to the naked eye. Two patients may appear similar in a traditional clinical assessment, yet present significant differences in their muscle activation.
This explains why, in some cases, functional classification may not fully reflect the patient’s actual performance.
Why EMG improves the way you assess
Electromyography (EMG) does not replace clinical judgment, but it adds a layer of objective information that allows for a much more precise assessment.
With EMG, you can identify whether a muscle is hyperactive at rest, whether there is an activation deficit during contraction, or whether there are relevant asymmetries between both sides.
This allows for a deeper understanding of the patient’s neuromuscular profile and supports more accurate decision-making.
Instead of relying solely on what you see, you can base your assessment on data that reflects what is actually happening inside the muscle.
When you understand the muscle’s real behavior, you can adapt training in a much more specific way.
You can work to reduce baseline hyperactivity, improve voluntary activation capacity, and optimize coordination between muscle groups.
Conclusion
In people with cerebral palsy, muscle alterations are not always obvious at first glance.
A muscle may appear functional, but be hyperactive at rest and inefficient during contraction. This pattern directly impacts performance, stability, and injury risk.
Electromyography allows you to detect these alterations with precision and transform the way you assess, train, and make clinical decisions.
Because in this context, observing movement is not enough.
You need to understand what is happening inside the muscle.

