Are you using the classic clamshell to work the gluteus medius of your patients?
If so, the muscle activation data measured with surface EMG is going to make you reconsider that exercise, or at least, at which stage of the programme it makes sense to use it.
Not all clamshell variations generate the same muscle response. The difference between the least effective option and the most effective one is 60% of contraction.
In terms of stimulus for the gluteus medius, that changes everything.
In this post you will learn 5 clamshell variations so you can start applying them with your patients today.
Why the gluteus medius matters more than it seems
The gluteus medius is the primary stabiliser of the pelvis in the frontal plane. Its deficit underlies some of the most common problems seen in clinical practice: knee valgus, iliotibial band syndrome, patellofemoral pain, gait alterations and hip and knee injuries in athletes.
The clamshell is one of the most widely used exercises to activate it because it requires no external load, is accessible at any stage of the rehabilitation process and has a straightforward execution.
The problem is that not all its variations are equally effective. And without EMG, there is no way to know which one is actually working for your patient.
Gluteus medius activation ranking by variation
🥇 1. Clamshell in four-point kneeling
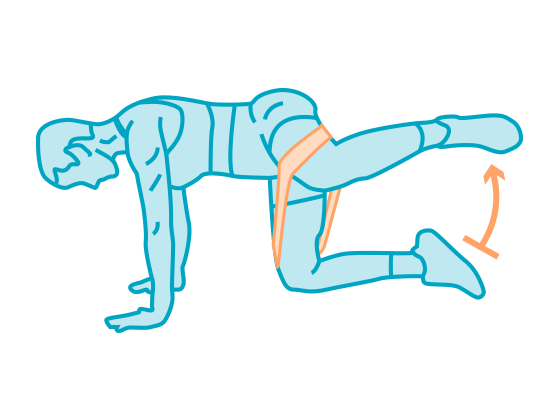
The most effective variation. In four-point kneeling, the hip position changes the working angle of the gluteus medius and considerably increases the demand on that muscle.
With 80% of its Maximum Voluntary Contraction (MVC), it is above the standard reference threshold for generating strength adaptations, making it the most appropriate option when the goal is to significantly strengthen the gluteus medius.
It is also the variation that demands the most from the patient in terms of postural control, so correct technique is required to direct the activation towards the gluteus medius and avoid compensation through lumbar rotation or trunk inclination.
🥈 2. Standing clamshell

The second most effective option reaches 70% MVC. The standing position introduces the variable of single-leg balance, which adds a stabilisation demand that better replicates real functional conditions: walking, running and changes of direction.
It is a good progression from the side-lying variations once the patient has sufficient control and the goal is to bring the exercise closer to more functional movement patterns.
🥉 3. Clamshell with side plank
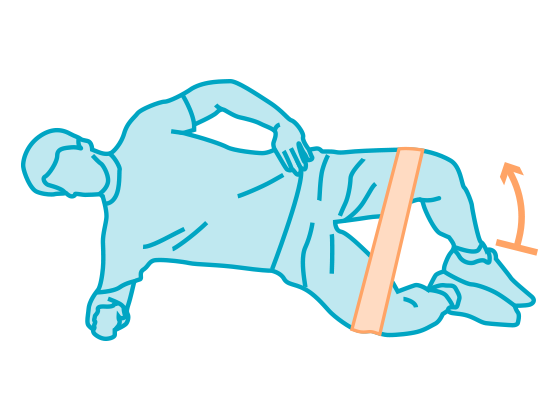
The side plank adds a trunk stabilisation demand that modifies the overall recruitment of the exercise.
With 40% MVC in the gluteus medius, it falls within a moderate range, useful in intermediate phases when the goal is to work core stability and hip abduction simultaneously.
4. Classic clamshell
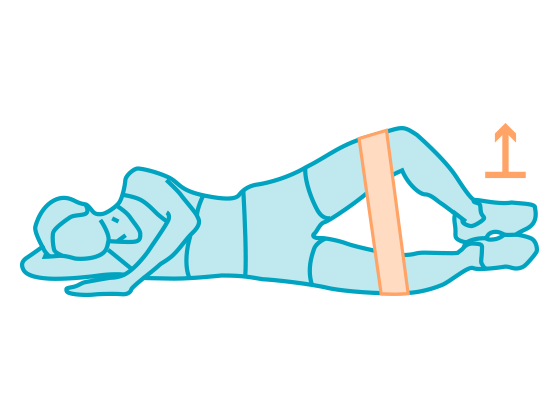
The classic side-lying clamshell, the most commonly used variation in clinical practice, only reaches 25% MVC in the gluteus medius. This is a low activation level if the goal is to generate strength adaptations.
It has its place in the very early stages of rehabilitation, when load tolerance is low or when the motor pattern needs to be taught before adding demand.
5. Clamshell with glute bridge
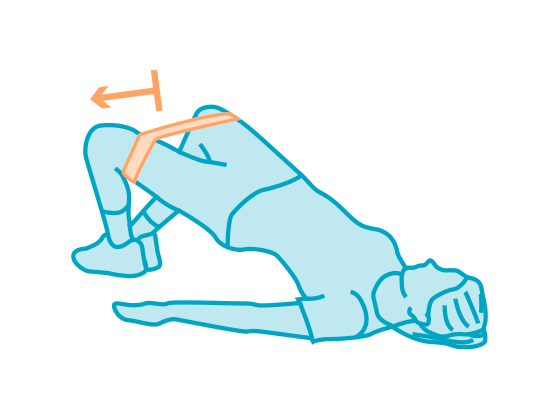
The combination of clamshell and glute bridge generates the lowest activation in the ranking: 20% MVC in the gluteus medius.
The glute bridge shifts the demand towards the gluteus maximus and the hamstrings, reducing the participation of the gluteus medius in hip abduction.
If the goal is to work the gluteus medius, this variation is not the most efficient. If the goal is to work the gluteus maximus with an added abduction component, it may make more sense.
How to interpret this data in your clinical practice
The ranking does not mean that the less active variations are useless. It means that each one has a different place in the rehabilitation process depending on the goal and the phase of treatment.
A logical progression based on this data:
- Early phase: classic clamshell to teach the motor pattern and tolerate the exercise without excessive demand.
- Intermediate phase: clamshell with side plank to add trunk stabilisation with moderate gluteus medius activation.
- Advanced phase: standing or four-point kneeling clamshell to reach activation levels sufficient for greater strength gains.
The problem is that without EMG you do not know what activation level your patient is really at in each phase.
Two patients can perform the same exercise with apparently similar technique and achieve completely different activation levels. EMG gives you that individual data point that population reference values from a study cannot provide.
Frequently asked questions
Is the classic clamshell useless? No, but it serves a specific purpose: teaching the motor pattern in early phases or working with patients who cannot tolerate greater demand. At 25% MVC it is not sufficient to generate significant strength adaptations in the gluteus medius in patients with basic functional capacity.
Why does the four-point kneeling clamshell activate the gluteus medius more than the classic version? In four-point kneeling, the hip position changes the working angle of the gluteus medius and modifies the length-tension relationships of the muscle. Additionally, the position demands greater active pelvic stabilisation, which increases gluteus medius recruitment as a stabiliser.
Are these values applicable to all patients? They are reference values measured with surface EMG in a specific sample. Real activation varies according to execution technique, fatigue level, recovery phase and individual characteristics. Individual measurement with EMG always provides more information than population data.
Can I use the standing clamshell in patients with knee pain? It depends on the cause of the pain and the patient’s tolerance. The single-leg position increases demand on the supporting knee. If there is joint irritability, the four-point kneeling clamshell is an alternative with similar activation but without knee loading.
Conclusion
The classic clamshell is one of the most commonly prescribed exercises for the gluteus medius, but at only 25% MVC it is also one of the least effective for strengthening it. The four-point kneeling and standing variations, at 80% and 70% MVC respectively, are considerably more efficient options and require no additional equipment.
Knowing this data allows you to design progressions with sound criteria: starting where it makes sense to start and advancing when the muscle is ready for greater demand.
And if you want to know exactly what level the gluteus medius of your specific patient is at, the answer lies in measuring it.

