And stop treating shoulder pain blindly
Many patients with shoulder pain come to the clinic convinced that they need to work on “strength.” They have tried exercises, trained with loads, and even improved certain movements, yet the pain keeps returning.
In many of these cases, the problem is not strength. The problem is scapular control.
The scapula is the foundation on which the shoulder moves. If that foundation is not stable and well-coordinated, any movement (pushing, pulling, or raising the arm) is performed on an inefficient structure.
The result is predictable: the patient loses control during pushing, loses stability during pulling, and the shoulder begins to compensate. Over time, this leads to pain, cervical overload, and functional limitations.
That’s why, before strengthening, you need to answer a key question: Is the scapula functioning properly?
Why assessing scapular control is essential
Clinical practice and evidence agree on one point: alterations in scapular movement (scapular dyskinesis) are closely related to shoulder pain.
In many patients, three very characteristic patterns appear. On one hand, inhibition of the serratus anterior, which prevents proper protraction and stabilization. On the other hand, a deficit in the lower trapezius, which compromises the ability to control the scapula during pulling and elevation movements. And, as a consequence, there is often overactivation of the upper trapezius, which attempts to compensate for this lack of control.
The problem is that these patterns are not always visible at first glance. The patient may complete the movement, but does so using a compensatory strategy.
Your job is not just to observe the movement. It is to understand which muscle is leading the action and which one is failing.
Practical 15-minute protocol
This protocol allows you to quickly and systematically assess scapular protraction and retraction control. You don’t need complex tests, but you do need to know what to observe and how to interpret it.
Test 1: High Retraction
This test analyzes the patient’s ability to control scapular retraction, especially the role of the lower trapezius.
In an efficient pattern, the lower trapezius should clearly contribute to scapular stabilization during pulling.However, in many patients, an altered synergy appears where the serratus anterior dominates the movement without proper stabilization from the lower trapezius.
A correct synergy means that the lower trapezius activates more than the serratus anterior.
Now look at this example:
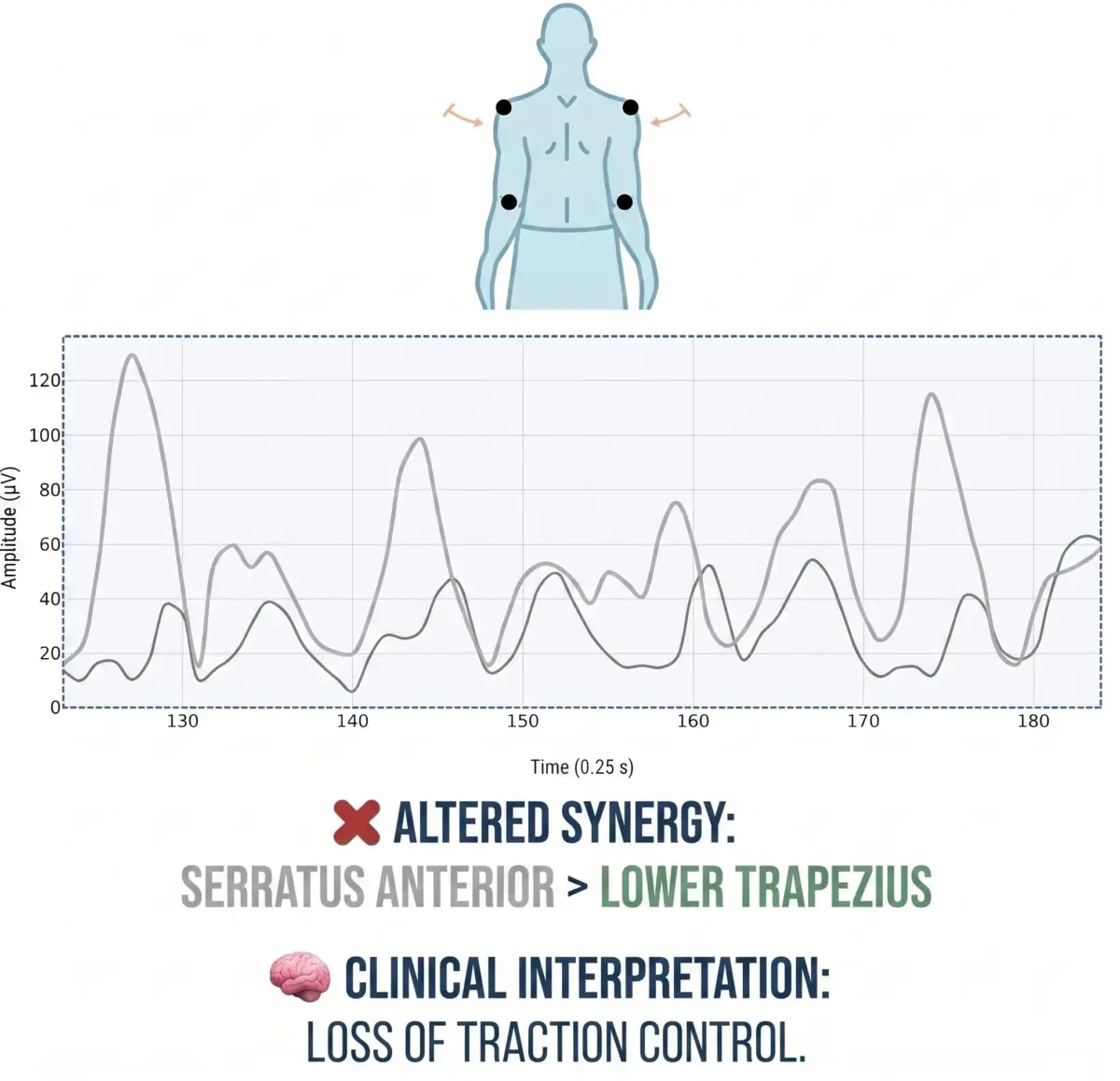
The lower trapezius activates less than the serratus anterior.
This results in a loss of control during pulling exercises. The patient can pull, but cannot properly stabilize the scapula.
The intervention here is not about adding more load, but about re-educating the pattern, helping the patient feel and activate the lower trapezius accurately.
Test 2: Push-ups on the wall or floor
This test evaluates scapular control during a pushing movement, where the serratus anterior should be the main contributor.
When the pattern is correct, the serratus anterior allows controlled protraction and keeps the scapula stable against the rib cage. However, in many cases, the opposite occurs: the lower trapezius or even the upper trapezius take over part of the work, while the serratus does not activate sufficiently.
In this case, a correct synergy means that the serratus anterior activates more than the lower trapezius.
Now look at this example:
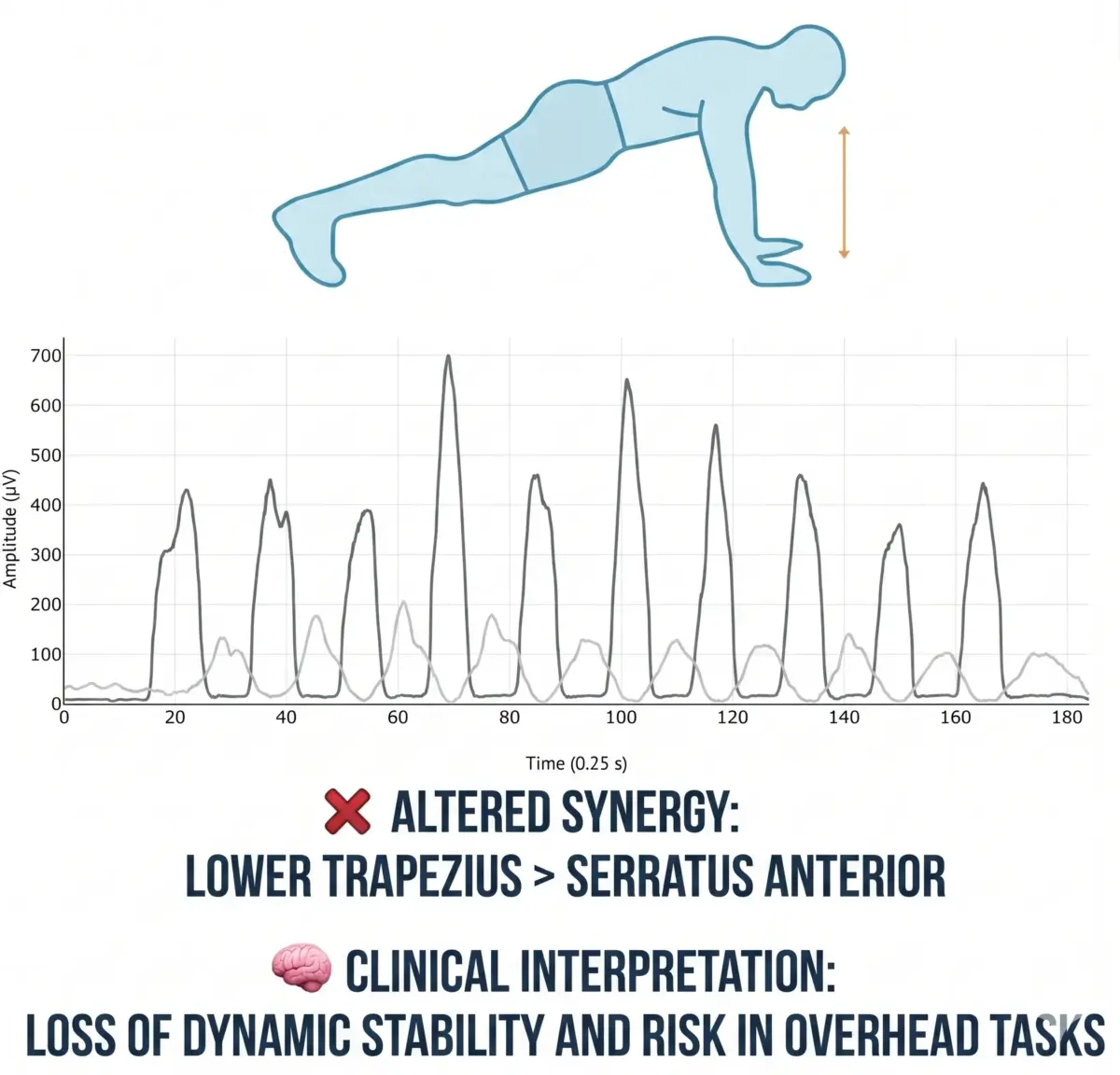
The serratus anterior activates less than the lower trapezius.
This leads to a loss of dynamic stability, especially in tasks where the arm works overhead.Here, the objective is clear: re-educate scapular protraction, prioritizing control over load. If the serratus does not lead the movement, the exercise is not fulfilling its function.
Test 3: Shoulder flexion
Arm elevation is one of the movements where scapular control becomes most evident.
During efficient shoulder flexion, the scapula must accompany the movement in a coordinated way, respecting the scapulohumeral rhythm. However, when this control fails, a very common pattern appears: the upper trapezius becomes overactive, excessively elevating the scapula, while the serratus anterior and lower trapezius do not participate enough.
In this example, an altered synergy appears because the upper trapezius is the most active muscle, above the serratus and the lower trapezius.
The result is an altered movement rhythm, often accompanied by cervical overload and discomfort during elevation.
In this case, the common mistake is trying to progress load without first correcting the pattern. The priority should be to restore scapular control before increasing shoulder demand.
What happens when scapular control fails
When the scapula is not properly controlled, the shoulder loses its foundation of stability.
This creates a cascade of compensations. The neck starts to contribute more than necessary, cervical tension appears, and the patient loses efficiency in pushing and pulling movements. In addition, the force the shoulder can generate decreases, because it lacks a stable base to work from.
Over time, this pattern leads to recurrent pain, especially in overhead movements or repetitive tasks.
On the other hand, when scapular control is adequate, everything changes. The scapula provides a stable base, the shoulder works more efficiently, and the risk of injury decreases.
Why measuring with EMG will improve your intervention
One of the biggest problems in shoulder assessment is that many decisions are based on observation and the patient’s subjective perception.
Electromyography (EMG) allows you to go one step further. It provides objective data on which muscle is activating, when it activates, and with what intensity.
You can verify whether the serratus anterior truly leads protraction or whether the lower trapezius is stabilizing the scapula during retraction. You can also see how this pattern changes after applying an intervention.
This allows you to make much more precise decisions: knowing when to progress, when to correct, and whether an exercise is achieving its goal.
Conclusion
Many shoulder problems are not due to a lack of strength, but to a lack of scapular control.
If you do not assess scapular protraction and retraction, it is easy to overlook the real source of the problem and reinforce compensations.
This protocol allows you to quickly identify which muscles are failing and how to intervene to correct the pattern.
Because in the shoulder, as in many other structures, it’s not just about moving… it’s about moving with the right muscle at the right time.
Here’s an important question: how much time are you spending strengthening the shoulder without knowing whether the scapula is stabilizing properly?

